

Surgical treatment of ruptured right middle cerebral artery mycotic aneurysm and central nervous system aspergillosis: Clinical case and literature review
- PMID: 34877041
- PMCID: PMC8645462
- DOI: 10.25259/SNI_843_2021
Surgical treatment of ruptured right middle cerebral artery mycotic aneurysm and central nervous system aspergillosis: Clinical case and literature review
Abstract
Background: Central nervous system (CNS) aspergillosis is more often met in patients with expressed immune suppression. Still, in 50% of cases of meningitis caused by Aspergillus spp., it is observed in patients without expressed immune suppression. The prognosis of CNS aspergillosis is unfavorable with the general rate of lethality around 70%.
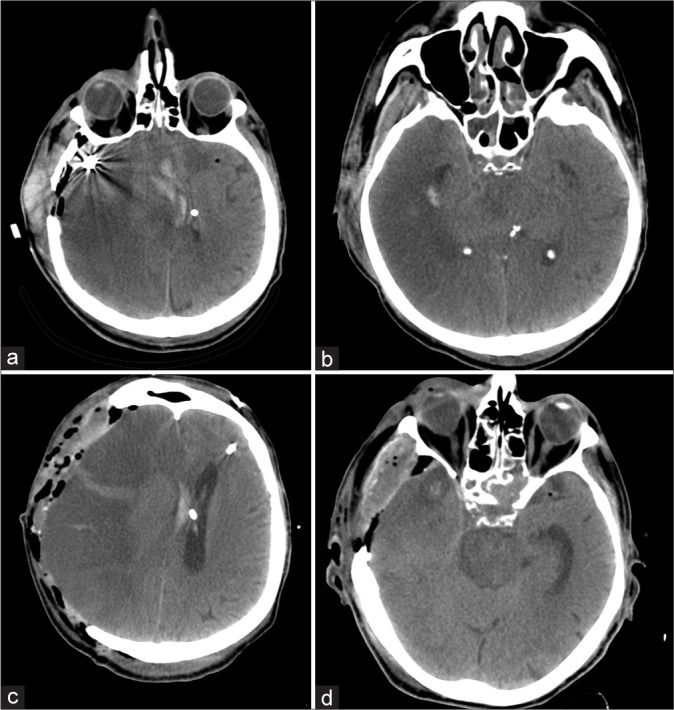
Case description: Clinical case of a 58-year-old man who developed an Aspergillus abscess in the chiasmosellar region and an associated mycotic aneurysm of the right middle cerebral artery (MCA) and intracerebral hemorrhage. Microsurgical clipping of the fusiform-ectatic aneurysm of the right MCA in the conditions of rupture was performed. An extra-intracranial micro anastomosis was formed on the right. An open biopsy of the neoplasm in the chiasmosellar region was made. The neoplasm was yellow and destroyed the bone plate of the skull base. Biopsy results: Mycotic lesion (aspergillosis). The analysis of surgical treatment for mycotic aneurysms in the acute period of hemorrhage in patients with aspergillosis revealed a high rate of lethality. The issue of the feasibility and effectiveness of complicated revascularization interventions in the patients with hemorrhage and aspergillosis remains unsolved.
Conclusion: The lack of generally accepted tactics of the treatment of this pathology requires further studies and systemic analysis. A high risk of the lethal outcome in patients with invasive mycotic infection and rupture of mycotic aneurysm highlight the importance of timely diagnostics and the beginning of antimycotic therapy. WThe issue of the evaluation of the revascularization methods effectiveness in patients after surgical treatment of a mycotic aneurysm associated with cerebral aspergillosis remains poor.
Keywords: Aspergillosis; Bypass; Ruptured aneurysm.
Copyright: © 2021 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures





References
-
- Baeesa SS, Bakhaidar M, Ahamed NA, Madani TA. Invasive orbital apex aspergillosis with mycotic aneurysm formation and subarachnoid hemorrhage in immunocompetent patients. World Neurosurg. 2017;102:42–8. - PubMed
-
- Bokhari R, Baeesa S, Al-Maghrabi J, Madani T. Isolated cerebral aspergillosis in immunocompetent patients. World Neurosurg. 2014;82:e325–33. - PubMed
-
- Jao SY, Weng HH, Wong HF, Wang WH, Tsai YH. Successful endovascular treatment of intractable epistaxis due to ruptured internal carotid artery pseudoaneurysm secondary to invasive fungal sinusitis. Head Neck. 2014;36:1391. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous