

Surgery for Cutaneous Squamous Cell Carcinoma and its Limits in Advanced Disease
- PMID: 34877075
- PMCID: PMC8609953
- DOI: 10.5826/dpc.11S2a167S
Surgery for Cutaneous Squamous Cell Carcinoma and its Limits in Advanced Disease
Abstract
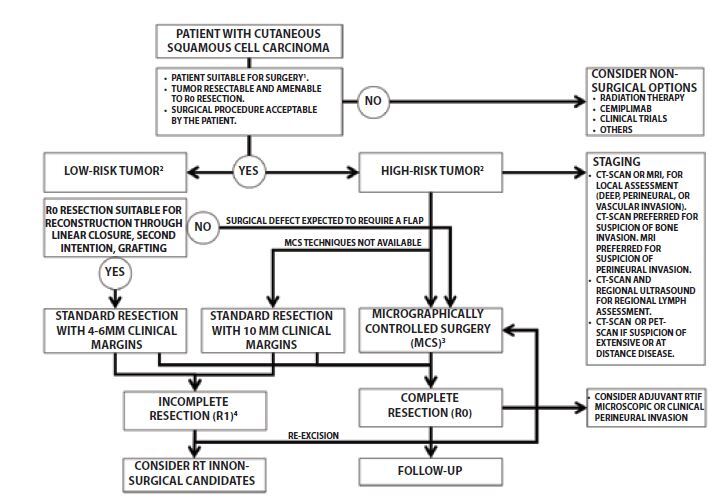
Surgery remains the first-line therapeutic option for most patients with cutaneous squamous cell carcinoma (cSCC). However, in the current therapeutic landscape, surgery must attempt to the complete tumor resection (R0 resection) with the lowest risk of surgical complications. This double aim is usually accomplished through standard excision with clinical margins in patients with low-risk tumors or by some of the micrographically controlled surgery procedures for patients with tumors at high-risk of local recurrence and metastasis. Surgery is also a first-line treatment for nodal metastases of cSCC as well as an option to consider in patients who develop recurrences while receiving immunotherapy, or as a palliation procedure in patients with advanced tumors. Neoadjuvant immunotherapy, that is the use of a medical treatment before surgery, is under investigation in patients with cSCC. The decision-making process and guidelines recommendations regarding cSCC surgery are reviewed in this manuscript.
Keywords: Mohs surgery; cutaneous squamous cell carcinoma; nodal metastases; nodal surgery; oncologic surgery; surgery.
©2021 Moreno-Ramírez et al.
Conflict of interest statement
Competing interests: None.
Figures


Similar articles
-
European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 2. Treatment.Eur J Cancer. 2020 Mar;128:83-102. doi: 10.1016/j.ejca.2020.01.008. Epub 2020 Feb 26. Eur J Cancer. 2020. PMID: 32113942
-
European consensus-based interdisciplinary guideline for invasive cutaneous squamous cell carcinoma: Part 2. Treatment-Update 2023.Eur J Cancer. 2023 Nov;193:113252. doi: 10.1016/j.ejca.2023.113252. Epub 2023 Jul 28. Eur J Cancer. 2023. PMID: 37708630
-
Non-melanoma skin cancer: United Kingdom National Multidisciplinary Guidelines.J Laryngol Otol. 2016 May;130(S2):S125-S132. doi: 10.1017/S0022215116000554. J Laryngol Otol. 2016. PMID: 27841126 Free PMC article.
-
Advanced or Metastatic Cutaneous Squamous Cell Carcinoma: The Current and Future Role of Radiation Therapy in the Era of Immunotherapy.Cancers (Basel). 2022 Apr 7;14(8):1871. doi: 10.3390/cancers14081871. Cancers (Basel). 2022. PMID: 35454779 Free PMC article. Review.
-
Case report: Patient specific combination of surgery and immunotherapy in advanced squamous cell carcinoma of the head and neck - a case series and review of literature.Front Immunol. 2022 Oct 27;13:970823. doi: 10.3389/fimmu.2022.970823. eCollection 2022. Front Immunol. 2022. PMID: 36389668 Free PMC article. Review.
Cited by
-
Facial Reconstruction After Total Resection of Long-Standing Cutaneous Squamous Cell Carcinoma.Cureus. 2024 Oct 19;16(10):e71864. doi: 10.7759/cureus.71864. eCollection 2024 Oct. Cureus. 2024. PMID: 39559683 Free PMC article.
-
Clinical and histopathological features of advanced cutaneous squamous cell carcinoma with varying responses to cemiplimab.J Dtsch Dermatol Ges. 2025 Jan;23(1):30-37. doi: 10.1111/ddg.15551. Epub 2024 Nov 3. J Dtsch Dermatol Ges. 2025. PMID: 39491790 Free PMC article.
-
Trends in cutaneous squamous cell carcinoma on the lip incidence and mortality in the United States, 2000-2019.Front Oncol. 2023 Apr 17;13:1111907. doi: 10.3389/fonc.2023.1111907. eCollection 2023. Front Oncol. 2023. PMID: 37139158 Free PMC article.
-
Managing Advanced Squamous Cell Carcinoma: A Guide for the Dermatology Clinician.J Clin Aesthet Dermatol. 2025 Aug;18(8):20-26. J Clin Aesthet Dermatol. 2025. PMID: 40843236 Free PMC article. Review.
-
Malignant Fungating Wounds in Locally Aggressive Cutaneous Squamous Cell Carcinoma: A Case Series.Cureus. 2025 Mar 24;17(3):e81114. doi: 10.7759/cureus.81114. eCollection 2025 Mar. Cureus. 2025. PMID: 40276457 Free PMC article.
References
-
- Squamous.pdf. [Accessed August 10, 2021]. https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf .
Publication types
LinkOut - more resources
Full Text Sources