

Imaging findings of vitamin deficiencies: are they forgotten diseases?
- PMID: 34877451
- PMCID: PMC8611688
- DOI: 10.1259/bjro.20210011
Imaging findings of vitamin deficiencies: are they forgotten diseases?
Abstract
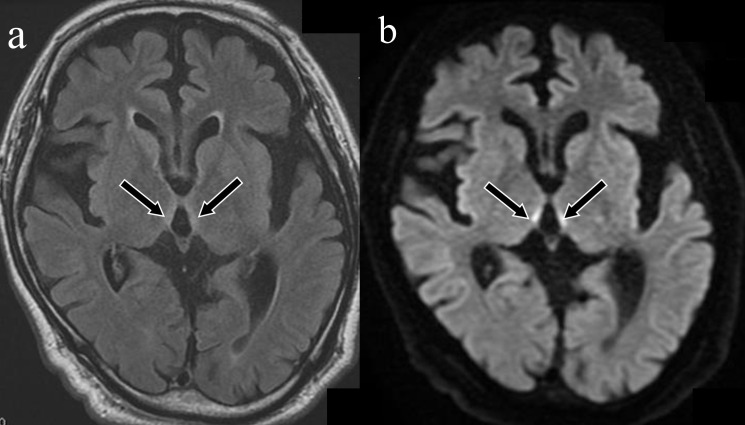
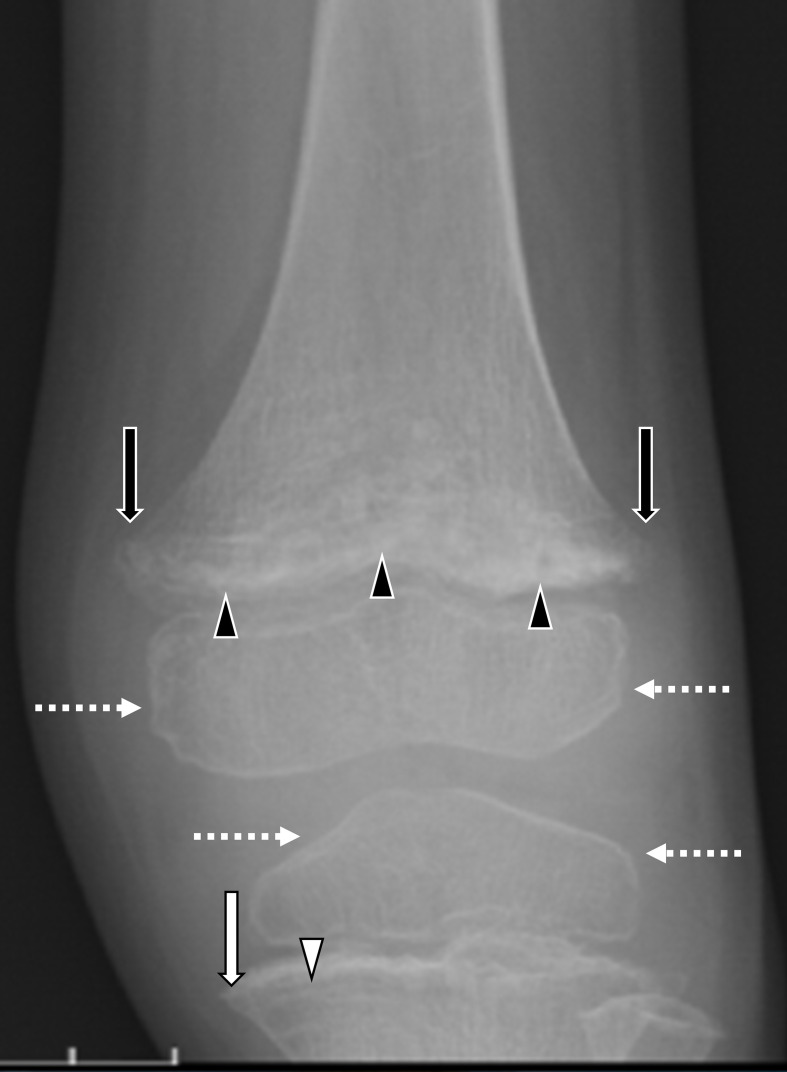
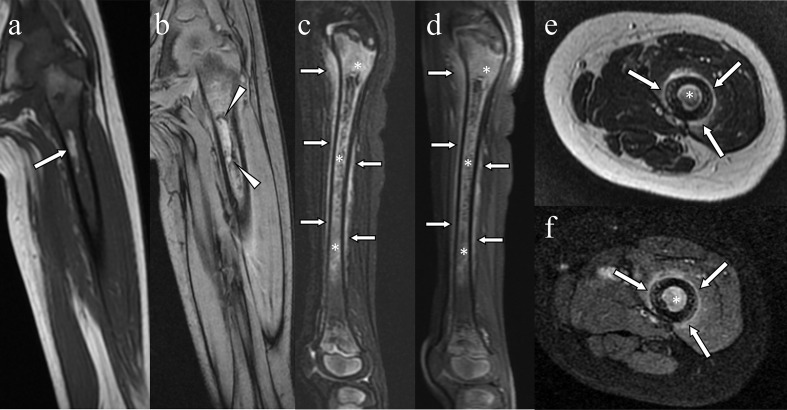
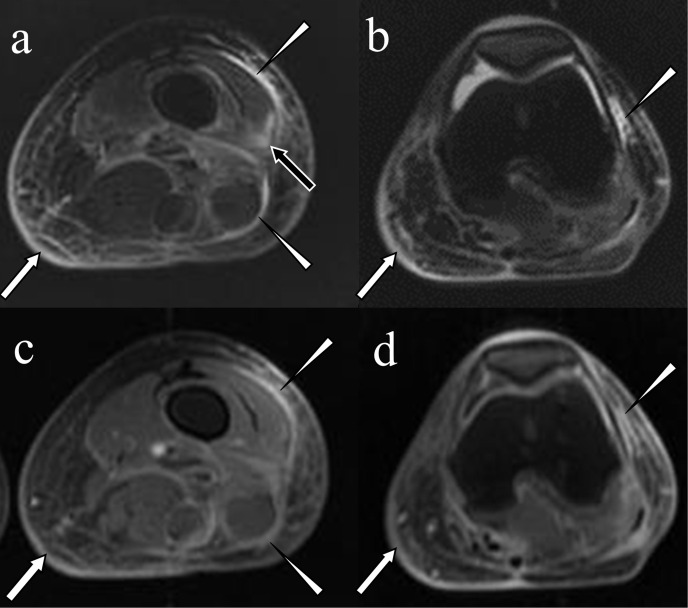
Vitamin deficiency is rare in modern industrialised countries; however, it still occurs in patients with specific backgrounds, such as those with extremely unbalanced diets, those with alcoholism and those who have undergone gastrointestinal surgery. Imaging examinations that demonstrate classic findings confirm the clinical diagnosis of vitamin deficiency and help monitor response to treatment. Because vitamin deficiencies are not prevalent, the diagnosis might not be straightforward. Therefore, imaging should be performed in cases of suspected vitamin deficiency. Radiologists should be familiar with characteristic imaging findings of vitamin deficiency and should survey an affected patient's background and blood vitamin levels. Because symptoms of vitamin deficiency are quickly improved by vitamin replacement, early diagnosis is essential. This pictorial review provides imaging findings for deficiencies in vitamins B1 (Wernicke encephalopathy and wet beriberi), B12 (subacute combined degeneration), C (scurvy), D (rickets) and K (bleeding tendency).
© 2021 The Authors. Published by the British Institute of Radiology.
Figures






References
Publication types
LinkOut - more resources
Full Text Sources
