

Emergency department-initiated buprenorphine protocols: A national evaluation
- PMID: 34877567
- PMCID: PMC8630357
- DOI: 10.1002/emp2.12606
Emergency department-initiated buprenorphine protocols: A national evaluation
Abstract
Objective: Emergency department-initiated buprenorphine (BUP) for opioid use disorder is an evidence-based practice, but limited data exist on BUP initiation practices in real-world settings. We sought to characterize protocols for BUP initiation among a geographically diverse sample of emergency departments (EDs).
Methods: In December 2020, we reviewed prestudy clinical BUP initiation protocols from all EDs participating in CTN0099 Emergency Department-INitiated bupreNOrphine VAlidaTION (ED-INNOVATION). We abstracted information on processes for identification of treatment-eligible patients, BUP administration, and discharge care.
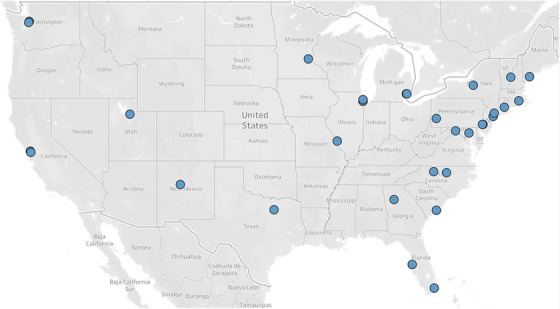
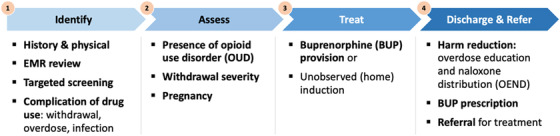
Results: All participating ED-INNOVATION sites across 22 states submitted protocols; 31 protocols were analyzed. Identification of treatment-eligible patients: Most EDs 22 (71%) relied on clinician judgment to determine appropriateness of BUP treatment with only 7 (23%) requiring decision support tools or diagnosis checklists. Before BUP initiation, 27 (87%) protocols required a documented Clinical Opiate Withdrawal Scale (COWS) score; 4 (13%) required a clinical diagnosis of withdrawal with optional COWS score. Twenty-seven (87%) recommended a minimum COWS score of 8 for ED-initiated BUP. BUP administration: Initial BUP dose ranged from 2-16 mg (mode = 4). For continued withdrawal symptoms, 27 (87%) protocols recommended an interval of 30-60 minutes between first and second BUP dose. Total BUP dose in the ED ranged from 8 to 32 mg. Discharge care: Twenty-eight (90%) protocols recommended a BUP prescription (mode 16 mg daily) at discharge. Naloxone prescription and/or provision was suggested in 23 (74%) protocols.
Conclusions: In this geographically diverse sample of EDs, protocols for ED-initiated BUP differed between sites. Future work should evaluate the association between this variation and patient outcomes.
Keywords: buprenorphine protocol; emergency department; opioid use disorder; opioid withdrawal.
© 2021 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of American College of Emergency Physicians.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ahmad FB, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics; 2021.
-
- The ASAM national practice guideline for the treatment of opioid use disorder: 2020 focused update. J Addict Med. 2020;14:1‐91. - PubMed
-
- Substance Abuse and Mental Health Service Administration . FAQs: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID‐19 emergency. National Mental Health and Substance Use Policy Laboratory. Substance Abuse and Mental Health Services Administration, 2020. https://www.samhsa.gov/sites/default/files/faqs‐for‐oudprescribing‐and‐d...
Grants and funding
LinkOut - more resources
Full Text Sources
