

Comparison of a Nasal Mask and Traditional Nasal Cannula During Intravenous Anesthesia for Gastroscopy Procedures: A Randomized Controlled Trial
- PMID: 34878412
- PMCID: PMC8826611
- DOI: 10.1213/ANE.0000000000005828
Comparison of a Nasal Mask and Traditional Nasal Cannula During Intravenous Anesthesia for Gastroscopy Procedures: A Randomized Controlled Trial
Abstract
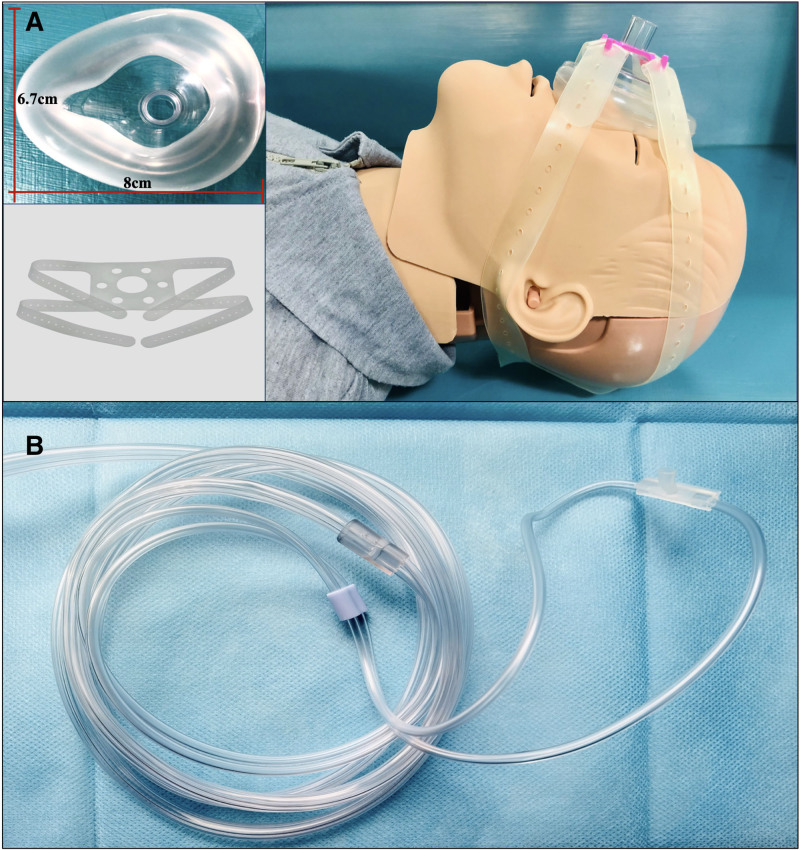
Background: Hypoxemia can occur during gastroscopy under intravenous anesthesia. The aim of this randomized controlled trial was to evaluate whether oxygenation using a nasal mask can reduce the incidence of hypoxemia during gastroscopy under intravenous anesthesia compared with a traditional nasal cannula.
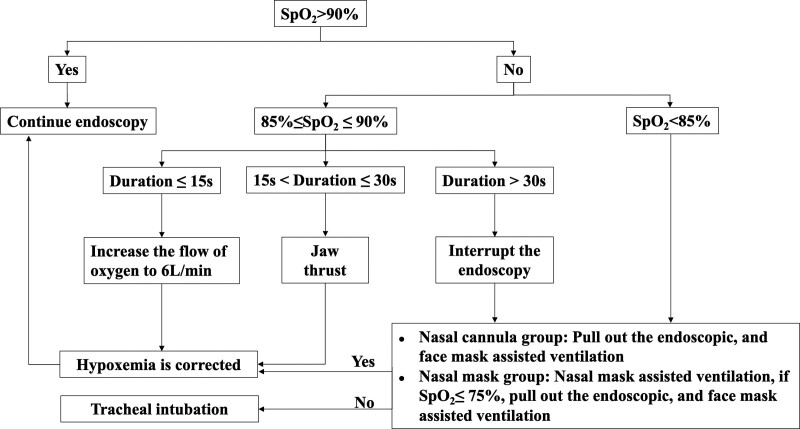
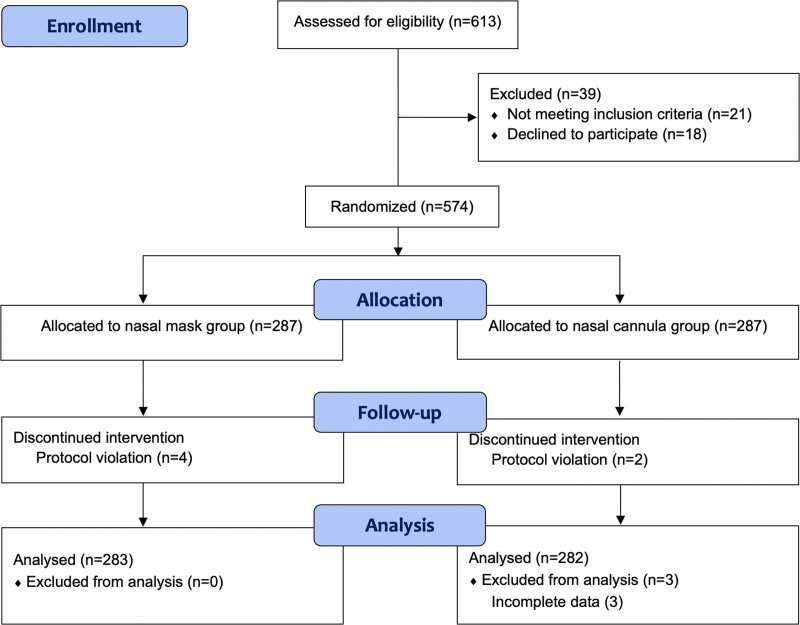
Methods: A total of 574 patients scheduled for gastroscopy under intravenous anesthesia were enrolled and randomly assigned to receive either a nasal mask or a traditional nasal cannula for oxygenation. The primary outcome was the incidence of hypoxemia. The secondary outcomes included the incidence of severe hypoxemia, duration of hypoxemia, minimum oxygen saturation, the proportion of emergency airway management, length of procedure, recovery time, and the satisfaction of the anesthetist and gastroenterologists as well as other adverse events (including cough, hiccups, nausea and vomiting, reflux, aspiration, and laryngospasm).
Results: A total of 565 patients were included in the analysis: 282 patients in the nasal cannula group and 283 patients in the nasal mask group. The incidence of hypoxemia was lower in the nasal mask group (18.0%) than in the nasal cannula group (27.7%; relative risk [RR] = 0.65; 95% confidence interval [CI], 0.48-0.89; P = .006), and the hypoxemia lasted a median of 18.0 seconds (interquartile range, 10.0-38.8) in the nasal mask group and 32.5 seconds (20.0-53.5) in the nasal cannula group (median difference -14.50; 95% CI, -22.82 to -1.34; P = .047). The proportion of patients requiring emergency airway management was significantly lower in the nasal mask group (8.8%) than in the nasal cannula group (19.1%; RR, 0.46; 95% CI, 0.30-0.73; P < .001). No difference was found in the overall incidence of other adverse events between the 2 groups (nasal mask 20.8%; nasal cannula 17.0%; RR, 1.23; 95% CI, 0.87-1.73; P = .25). Satisfaction was higher with the nasal mask than with the nasal cannula from the perspective of anesthetists (96.1% for nasal mask versus 84.4% for nasal cannula; RR, 1.14; 95% CI, 1.08-1.20; P < .001) and gastroenterologists (95.4% for mask versus 81.9% for cannula; RR, 1.17; 95% CI, 1.10-1.24; P < .001). There were no significant differences in the incidence of severe hypoxemia, minimum oxygen saturation, length of procedure, or recovery time between the 2 groups.
Conclusions: Nasal mask oxygenation reduced the incidence of hypoxemia during anesthesia for gastroscopy under intravenous anesthesia.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Anesthesia Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Comparison of a Nasal Mask and Traditional Nasal Cannula During Gastroscopy Procedures.Anesth Analg. 2022 Nov 1;135(5):e33. doi: 10.1213/ANE.0000000000006140. Epub 2022 Oct 21. Anesth Analg. 2022. PMID: 36269989 No abstract available.
Similar articles
-
Effects of anesthetic nasal masks on hypoxemia in overweight/obese patients undergoing gastroscopy: a randomized controlled trial.Eur J Med Res. 2025 May 2;30(1):355. doi: 10.1186/s40001-025-02534-2. Eur J Med Res. 2025. PMID: 40312693 Free PMC article. Clinical Trial.
-
High-flow nasal cannula oxygen reduced hypoxemia in patients undergoing gastroscopy under general anesthesia at ultra-high altitude: a randomized controlled trial.BMC Anesthesiol. 2024 May 27;24(1):189. doi: 10.1186/s12871-024-02568-9. BMC Anesthesiol. 2024. PMID: 38802783 Free PMC article. Clinical Trial.
-
Effect of nasal mask oxygenation on incidence of hypoxemia during gastroscopy with propofol sedation in patients at risk of hypoxemia: a prospective randomized controlled study.BMC Anesthesiol. 2025 Jul 30;25(1):366. doi: 10.1186/s12871-025-03245-1. BMC Anesthesiol. 2025. PMID: 40739469 Free PMC article. Clinical Trial.
-
The effectiveness of high-flow nasal cannula during sedated digestive endoscopy: a systematic review and meta-analysis.Eur J Med Res. 2022 Feb 24;27(1):30. doi: 10.1186/s40001-022-00661-8. Eur J Med Res. 2022. PMID: 35209948 Free PMC article.
-
Efficacy of high flow nasal oxygenation against hypoxemia in sedated patients receiving gastrointestinal endoscopic procedures: A systematic review and meta-analysis.J Clin Anesth. 2022 May;77:110651. doi: 10.1016/j.jclinane.2022.110651. Epub 2022 Jan 12. J Clin Anesth. 2022. PMID: 35030538
Cited by
-
Efficacy of high-flow nasal oxygen in preventing hypoxia during Gastrointestinal endoscopy: a retrospective cohort study.BMC Anesthesiol. 2025 Jun 3;25(1):287. doi: 10.1186/s12871-025-03155-2. BMC Anesthesiol. 2025. PMID: 40461980 Free PMC article.
-
Intravenous lidocaine decreased oxygen-desaturation episodes induced by propofol-based sedation for gastrointestinal endoscopy procedures: a prospective, randomized, controlled trial.BMC Anesthesiol. 2025 Jan 11;25(1):27. doi: 10.1186/s12871-025-02890-w. BMC Anesthesiol. 2025. PMID: 39799289 Free PMC article. Clinical Trial.
-
Bilevel positive airway pressure ventilation to prevent hypoxaemia during gastroscopy under sedation in patients at risk of hypoxaemia: study protocol for a prospective randomised controlled trial.BMJ Open. 2025 Mar 12;15(3):e096800. doi: 10.1136/bmjopen-2024-096800. BMJ Open. 2025. PMID: 40074253 Free PMC article.
-
Effects of anesthetic nasal masks on hypoxemia in overweight/obese patients undergoing gastroscopy: a randomized controlled trial.Eur J Med Res. 2025 May 2;30(1):355. doi: 10.1186/s40001-025-02534-2. Eur J Med Res. 2025. PMID: 40312693 Free PMC article. Clinical Trial.
-
Efficacy of nasal clips combined with nasal cannulas in preventing hypoxemia during gastrointestinal endoscopy with sedation: a randomized controlled trial.BMC Anesthesiol. 2025 Feb 19;25(1):83. doi: 10.1186/s12871-024-02863-5. BMC Anesthesiol. 2025. PMID: 39972293 Free PMC article. Clinical Trial.
References
-
- Inadomi JM, Gunnarsson CL, Rizzo JA, Fang H. Projected increased growth rate of anesthesia professional-delivered sedation for colonoscopy and EGD in the United States: 2009 to 2015. Gastrointest Endosc. 2010;72:580–586. - PubMed
-
- Qadeer MA, Lopez AR, Dumot JA, Vargo JJ. Hypoxemia during moderate sedation for gastrointestinal endoscopy: causes and associations. Digestion. 2011;84:37–45. - PubMed
