

Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes
- PMID: 34878511
- PMCID: PMC8655669
- DOI: 10.1001/jamasurg.2021.6339
Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes
Abstract
Importance: Surgeon sex is associated with differential postoperative outcomes, though the mechanism remains unclear. Sex concordance of surgeons and patients may represent a potential mechanism, given prior associations with physician-patient relationships.
Objective: To examine the association between surgeon-patient sex discordance and postoperative outcomes.
Design, setting, and participants: In this population-based, retrospective cohort study, adult patients 18 years and older undergoing one of 21 common elective or emergent surgical procedures in Ontario, Canada, from 2007 to 2019 were analyzed. Data were analyzed from November 2020 to March 2021.
Exposures: Surgeon-patient sex concordance (male surgeon with male patient, female surgeon with female patient) or discordance (male surgeon with female patient, female surgeon with male patient), operationalized as a binary (discordant vs concordant) and 4-level categorical variable.
Main outcomes and measures: Adverse postoperative outcome, defined as death, readmission, or complication within 30-day following surgery. Secondary outcomes assessed each of these metrics individually. Generalized estimating equations with clustering at the level of the surgical procedure were used to account for differences between procedures, and subgroup analyses were performed according to procedure, patient, surgeon, and hospital characteristics.
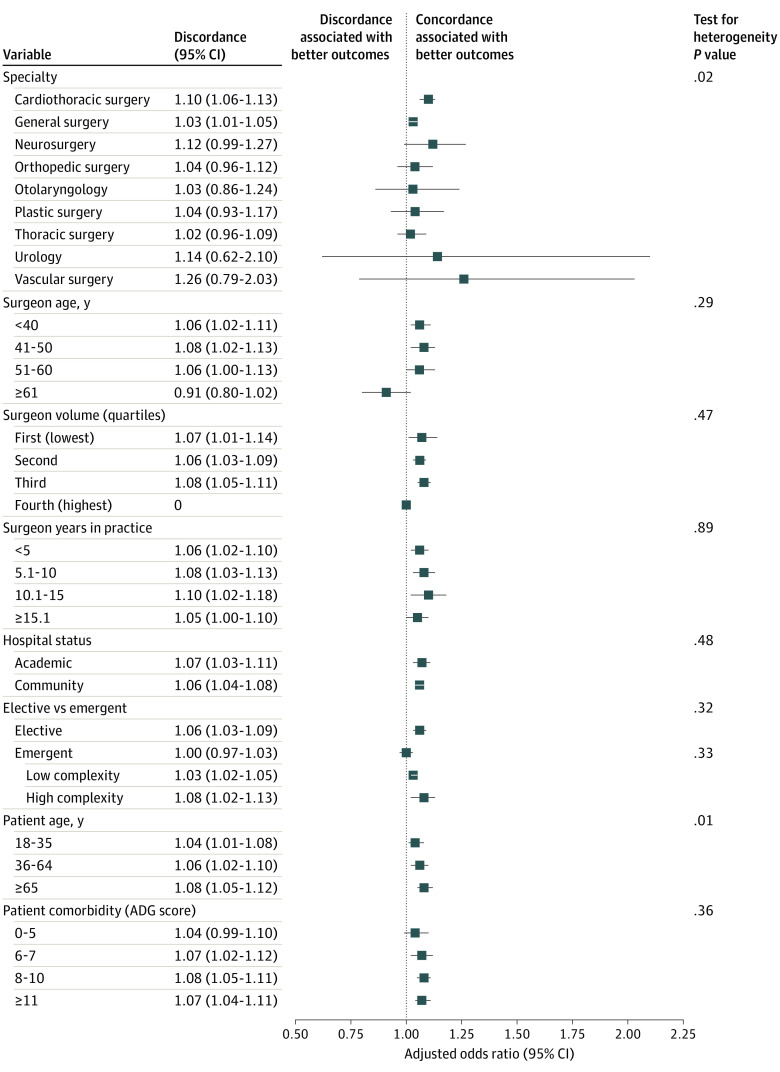
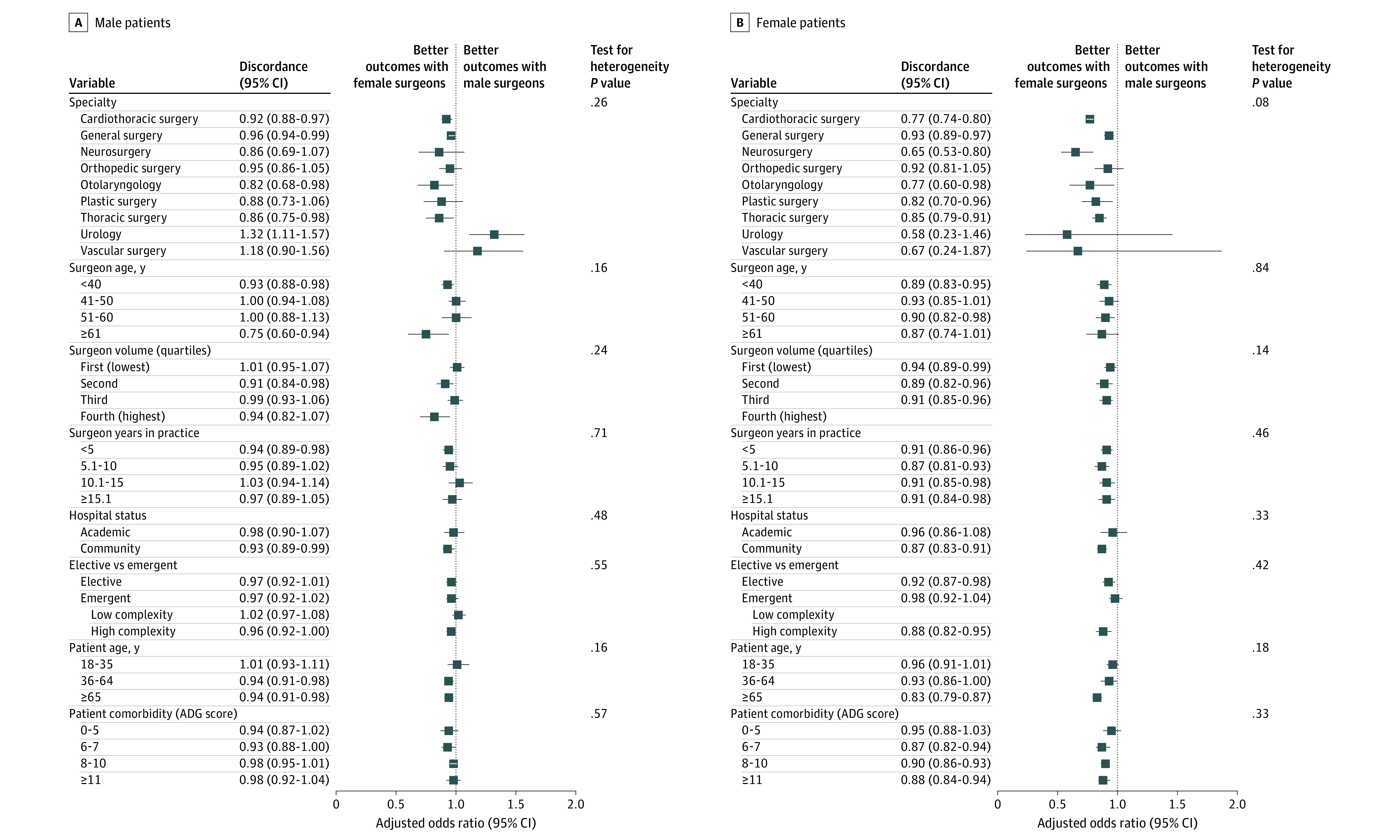
Results: Among 1 320 108 patients treated by 2937 surgeons, 602 560 patients were sex concordant with their surgeon (male surgeon with male patient, 509 634; female surgeon with female patient, 92 926) while 717 548 were sex discordant (male surgeon with female patient, 667 279; female surgeon with male patient, 50 269). A total of 189 390 patients (14.9%) experienced 1 or more adverse postoperative outcomes. Sex discordance between surgeon and patient was associated with a significant increased likelihood of composite adverse postoperative outcomes (adjusted odds ratio [aOR], 1.07; 95% CI, 1.04-1.09), as well as death (aOR, 1.07; 95% CI, 1.02-1.13), and complications (aOR, 1.09; 95% CI, 1.07-1.11) but not readmission (aOR, 1.02; 95% CI, 0.98-1.07). While associations were consistent across most subgroups, patient sex significantly modified this association, with worse outcomes for female patients treated by male surgeons (compared with female patients treated by female surgeons: aOR, 1.15; 95% CI, 1.10-1.20) but not male patients treated by female surgeons (compared with male patients treated by male surgeons: aOR, 0.99; 95% CI, 0.95-1.03) (P for interaction = .004).
Conclusions and relevance: In this study, sex discordance between surgeons and patients negatively affected outcomes following common procedures. Subgroup analyses demonstrate that this is driven by worse outcomes among female patients treated by male surgeons. Further work should seek to understand the underlying mechanism.
Conflict of interest statement
Figures
Comment in
-
Surgical Outcomes Should Know No Identity-The Case for Equity Between Patients and Surgeons.JAMA Surg. 2022 Feb 1;157(2):156-157. doi: 10.1001/jamasurg.2021.6367. JAMA Surg. 2022. PMID: 34878505 Free PMC article. No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes.JAMA Surg. 2022 Jul 1;157(7):639. doi: 10.1001/jamasurg.2022.0296. JAMA Surg. 2022. PMID: 35319733 No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes-Reply.JAMA Surg. 2022 Jul 1;157(7):639-640. doi: 10.1001/jamasurg.2022.0297. JAMA Surg. 2022. PMID: 35319734 No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes.JAMA Surg. 2022 Jul 1;157(7):637-638. doi: 10.1001/jamasurg.2022.0293. JAMA Surg. 2022. PMID: 35319742 No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes.JAMA Surg. 2022 Jul 1;157(7):638. doi: 10.1001/jamasurg.2022.0294. JAMA Surg. 2022. PMID: 35319745 No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes.JAMA Surg. 2022 Jul 1;157(7):636-637. doi: 10.1001/jamasurg.2022.0292. JAMA Surg. 2022. PMID: 35319752 No abstract available.
-
Comments on Surgeon-Patient Sex Concordance and Postoperative Outcomes.JAMA Surg. 2022 Jul 1;157(7):638-639. doi: 10.1001/jamasurg.2022.0295. JAMA Surg. 2022. PMID: 35319753 No abstract available.
References
-
- Malhotra J, Rotter D, Tsui J, Llanos AAM, Balasubramanian BA, Demissie K. Impact of patient-provider race, ethnicity, and gender concordance on cancer screening: findings from Medical Expenditure Panel Survey. Cancer Epidemiol Biomarkers Prev. 2017;26(12):1804-1811. doi:10.1158/1055-9965.EPI-17-0660 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
