

Stratified Care vs Stepped Care for Depression: A Cluster Randomized Clinical Trial
- PMID: 34878526
- PMCID: PMC8655665
- DOI: 10.1001/jamapsychiatry.2021.3539
Stratified Care vs Stepped Care for Depression: A Cluster Randomized Clinical Trial
Abstract
Importance: Depression is a major cause of disability worldwide. Although empirically supported treatments are available, there is scarce evidence on how to effectively personalize psychological treatment selection.
Objective: To compare the clinical effectiveness and cost-effectiveness of 2 treatment selection strategies: stepped care and stratified care.
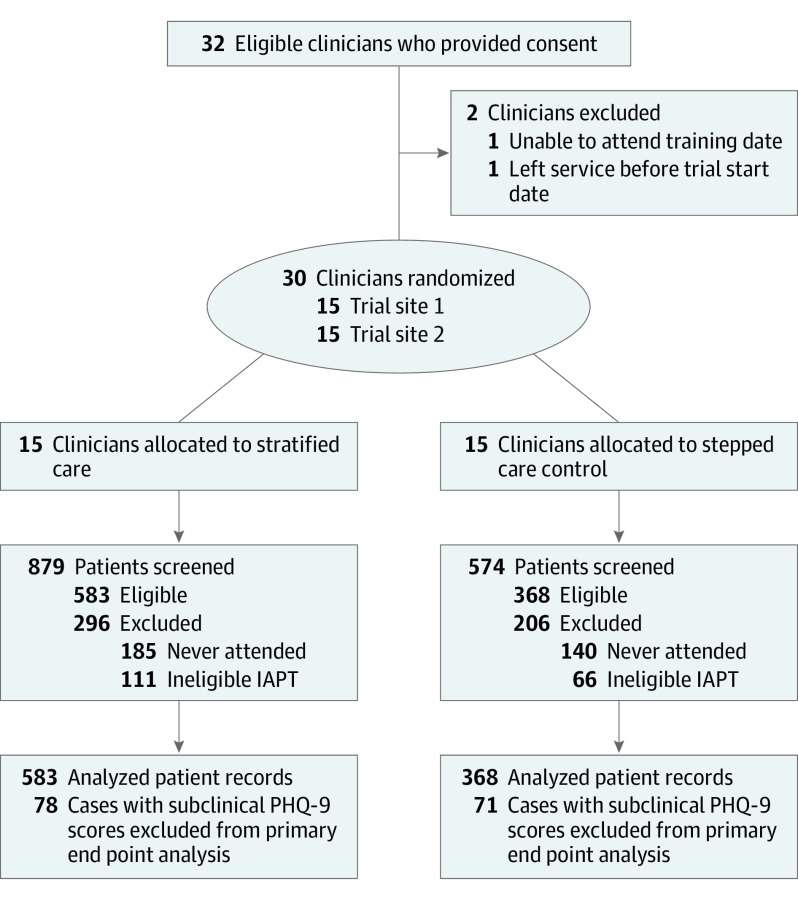
Design, setting, and participants: This multisite, cluster randomized clinical trial recruited participants from the English National Health Service from July 5, 2018, to February 1, 2019. Thirty clinicians working across 4 psychological therapy services were randomly assigned to provide stratified (n = 15) or stepped (n = 15) care. In stepped care, patients sequentially access low-intensity guided self-help followed by high-intensity psychotherapy. In stratified care, patients are matched with either low- or high-intensity treatments at initial assessment. Data were analyzed from May 18, 2020, to October 13, 2021, using intention-to-treat principles.
Interventions: All clinicians used the same interview schedule to conduct initial assessments with patients seeking psychological treatment for common mental disorders, but those in the stratified care group received a personalized treatment recommendation for each patient generated by a machine learning algorithm. Eligible patients received either stratified or stepped care (ie, treatment as usual).
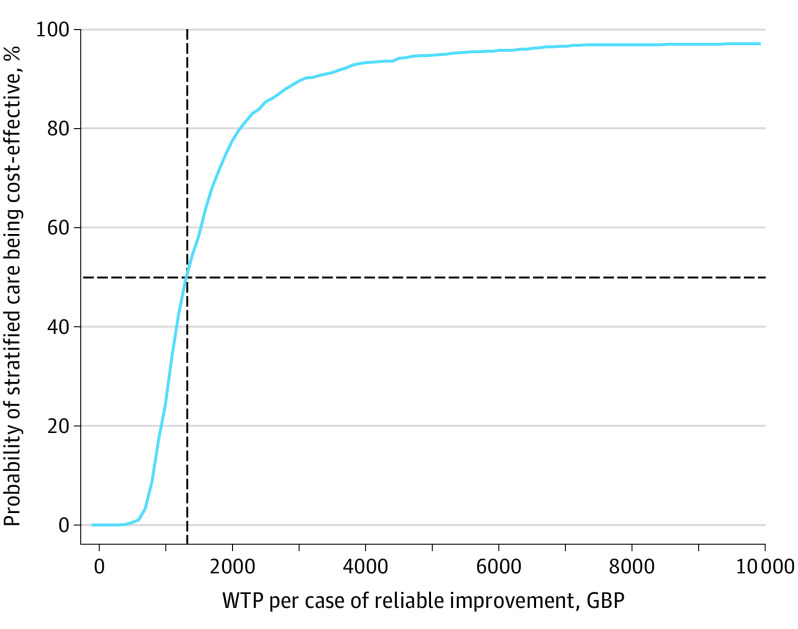
Main outcomes and measures: The preregistered outcome was posttreatment reliable and clinically significant improvement (RCSI) of depression symptoms (measured using the 9-item Patient Health Questionnaire). The RCSI outcome was compared between groups using logistic regression adjusted for baseline severity. Cost-effectiveness analyses compared incremental costs and health outcomes of the 2 treatment pathways.
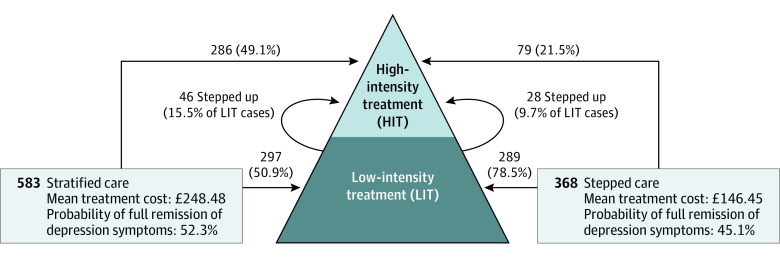
Results: A total of 951 patients were included (618 women among 950 with data available [65.1%]; mean [SD] age, 38.27 [14.53] years). The proportion of cases of RCSI was significantly higher in the stratified care arm compared with the stepped care arm (264 of 505 [52.3%] vs 134 of 297 [45.1%]; odds ratio, 1.40 [95% CI, 1.04-1.87]; P = .03). Stratified care was associated with a higher mean additional cost per patient (£104.5 [95% CI, £67.5-£141.6] [$139.83 (95% CI, $90.32-$189.48)]; P < .001) because more patients accessed high-intensity treatments (332 of 583 [56.9%] vs 107 of 368 [29.1%]; χ2 = 70.51; P < .001), but this additional cost resulted in an approximately 7% increase in the probability of RCSI.
Conclusions and relevance: In this cluster randomized clinical trial of adults with common mental disorders, stratified care was efficacious and cost-effective for the treatment of depression symptoms compared with stepped care. Stratified care can improve depression treatment outcomes at a modest additional cost.
Trial registration: isrctn.org Identifier: ISRCTN11106183.
Conflict of interest statement
Figures
References
-
- National Institute for Health and Care Excellence . Common mental health disorders: identification and pathways to care: clinical guidance [CG123]. May 25, 2011. Accessed January 6, 2021. https://www.nice.org.uk/guidance/CG123
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
