

Frequency of New Silent MRI Lesions in Myelin Oligodendrocyte Glycoprotein Antibody Disease and Aquaporin-4 Antibody Neuromyelitis Optica Spectrum Disorder
- PMID: 34878547
- PMCID: PMC8655599
- DOI: 10.1001/jamanetworkopen.2021.37833
Frequency of New Silent MRI Lesions in Myelin Oligodendrocyte Glycoprotein Antibody Disease and Aquaporin-4 Antibody Neuromyelitis Optica Spectrum Disorder
Abstract
Importance: In multiple sclerosis, magnetic resonance imaging (MRI) new silent lesions contribute to the diagnostic criteria, have prognostic value, and are used in treatment monitoring; but in aquaporin-4 antibody neuromyelitis optica spectrum disorder (AQP4-NMOSD), they are rare between attacks. Their frequency and their association with relapses in adults with myelin oligodendrocyte glycoprotein antibody disease (MOGAD) are still unclear.
Objective: To examine the frequency and characteristics of MRI new silent lesions in MOGAD and AQP4-NMOSD.
Design, setting, and participants: This retrospective cohort study analyzed clinical and MRI data of 404 patients with MOGAD or AQP4-NMOSD between February 1, 1994, and April 1, 2021; data were prospectively recorded on the Oxford NMOSD clinical database under follow-up. The study was conducted at the Oxford National Referral Center for NMOSD. Participants included patients with MOGAD and AQP4-NMOSD who were treated within the Oxford National NMO Specialist Service.
Exposures: Seropositive MOGAD and AQP4-NMOSD patients who had MRIs during attacks and the remission phase of their disease.
Main outcomes and measures: Frequency of new silent lesions detected by either attack MRIs (during the acute clinical event) or remission MRIs (performed outside of a relapse and at least 3 months from last attack). Median time to next relapse in the presence of definite (reference MRI performed at least 4 weeks from last attack onset), probable (reference MRI performed during last attack), and no new silent lesions on remission MRIs was also evaluated.
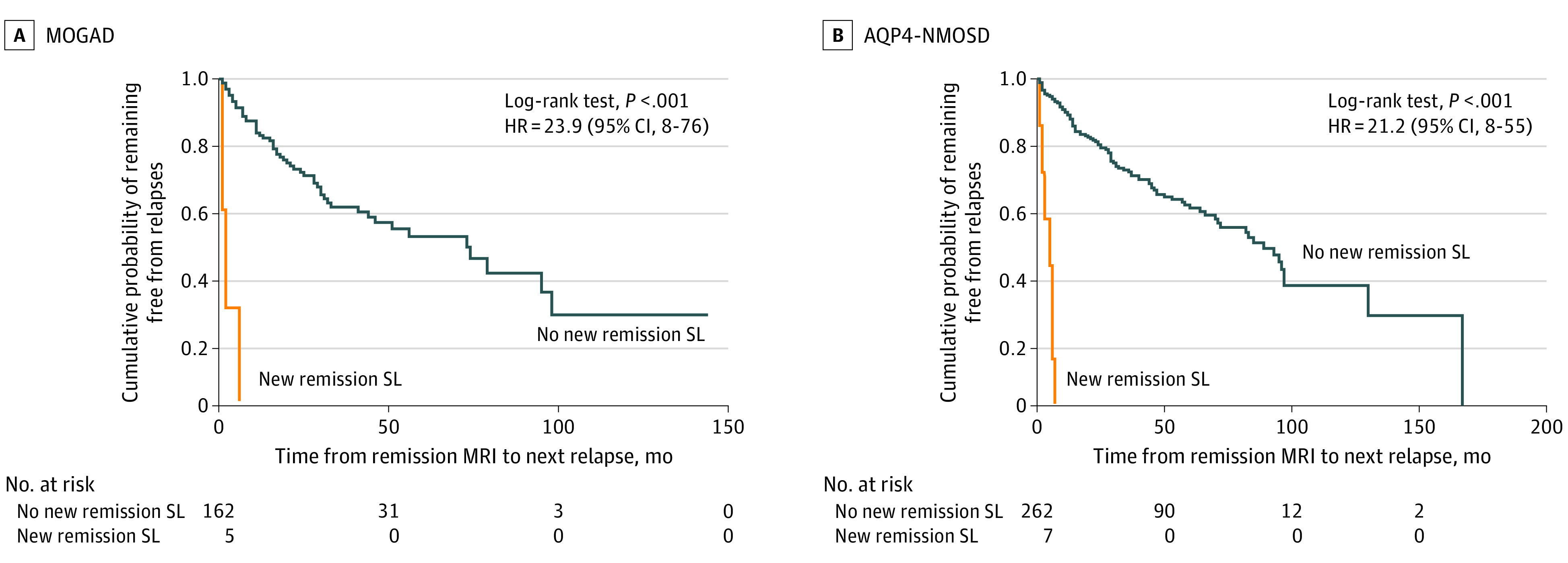
Results: One hundred eighty-two MOGAD patients and 222 AQP4-NMOSD patients were included. Of the MOGAD patients, 113 (62%) were female, median age at onset was 28 years (range, 2-72), and median follow-up was 52 months (range, 11-253). Of the AQP4-NMOSD patients, 189 (85%) were female, median age at onset was 43 years (range, 2-82), and median follow-up was 87.5 months (range, 11-260). MOGAD patients had 296 attack MRI sessions and 167 remission MRI sessions. New attack silent lesions were found in 97 of 296 (33%) attack MRI sessions, whereas new remission silent lesions were found in 5 of 167 (3.0%) remission MRI sessions. Median time from remission scan to the next relapse in the presence of definite or probable new remission lesions was 2 months (IQR, 1-6), whereas in the absence of any new remission lesions it was 73 months (IQR, 20-104; hazard ratio, 23.86; 95% CI, 7.51-75.79; P < .001). AQP4-NMOSD patients had 470 attack MRI sessions and 269 remission MRI sessions. New attack silent lesions were detected in 88 of 470 (18.7%) attack MRI sessions, whereas new remission silent lesions were found in 7 of 269 (2.6%) remission MRI sessions. Median time from remission scan to the next relapse in the presence of definite or probable new remission lesions was 5 months (IQR, 2-6), whereas in the absence of any new remission lesions it was 85 months (IQR, 29-167; hazard ratio, 21.23; 95% CI, 8.05-53.65; P < .001).
Conclusions and relevance: In contrast to that reported in multiple sclerosis, results of this cohort study suggest that new remission silent lesions are rare on follow-up scans in MOGAD and AQP4-NMOSD and appear to indicate a high risk of imminent relapse.
Conflict of interest statement
Figures
References
-
- Bruijstens AL, Lechner C, Flet-Berliac L, et al. ; EU Paediatric MOG Consortium . EU Paediatric MOG Consortium consensus, part 1: classification of clinical phenotypes of paediatric myelin oligodendrocyte glycoprotein antibody-associated disorders. Eur J Paediatr Neurol. 2020;29:2-13. doi:10.1016/j.ejpn.2020.10.006 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
