

Current and Emerging Classes of Pharmacological Agents for the Management of Hypertension
- PMID: 34878631
- PMCID: PMC8651502
- DOI: 10.1007/s40256-021-00510-9
Current and Emerging Classes of Pharmacological Agents for the Management of Hypertension
Abstract
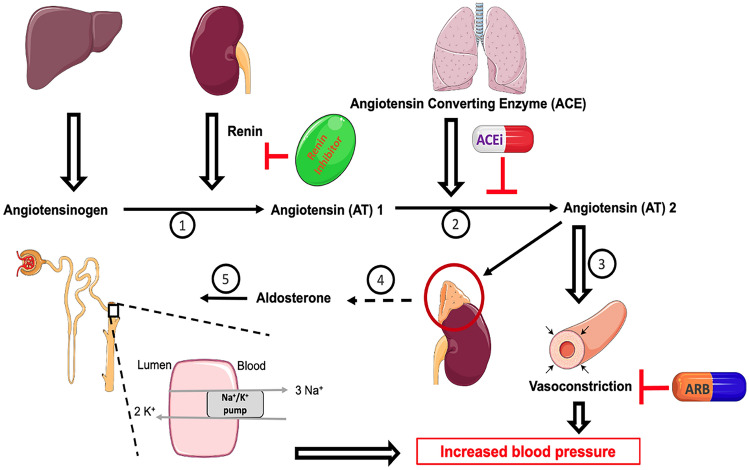
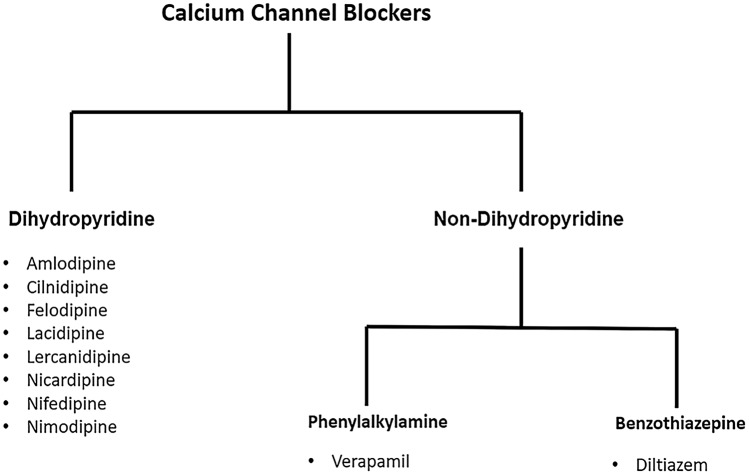
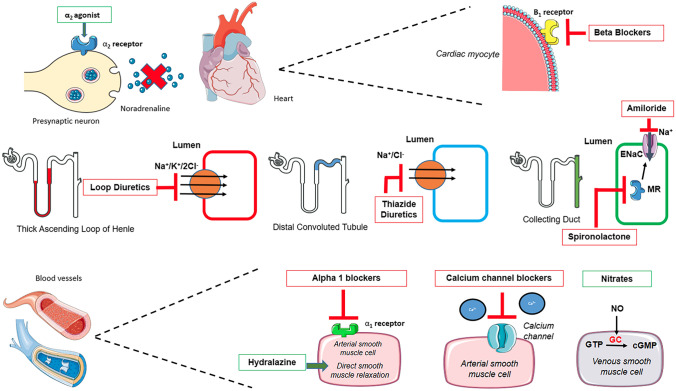
Cardiovascular disease accounts for more than 17 million deaths globally every year, of which complications of hypertension account for 9.4 million deaths worldwide. Early detection and management of hypertension can prevent costly interventions, including dialysis and cardiac surgery. Non-pharmacological approaches for managing hypertension commonly involve lifestyle modification, including exercise and dietary regulations such as reducing salt and fluid intake; however, a majority of patients will eventually require antihypertensive medications. In 2020, the International Society of Hypertension published worldwide guidelines in its efforts to reduce the global prevalence of raised blood pressure (BP) in adults aged 18 years or over. Currently, several classes of medications are used to control hypertension, either as mono- or combination therapy depending on the disease severity. These drug classes include those that target the renin-angiotensin-aldosterone system (RAAS) and adrenergic receptors, calcium channel blockers, diuretics and vasodilators. While some of these classes of medications have shown significant benefits in controlling BP and reducing cardiovascular mortality, the prevalence of hypertension remains high. Significant efforts have been made in developing new classes of drugs that lower BP; these medications exert their therapeutic benefits through different pathways and mechanism of actions. With several of these emerging classes in phase III clinical trials, it is hoped that the discovery of these novel therapeutic avenues will aid in reducing the global burden of hypertension.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
Utkarsh Ojha, Sanjay Ruddaraju, Navukkarasu Sabapathy, Varun Ravindran, Pitchaya Worapongsatitaya, Jeesanul Haq, Raihan Mohammed and Vinod Patel have no conflicts of interest to declare.
Figures
References
-
- Whelton P, Carey R, Aronow W, Casey D, Collins K, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018;71(19):e127–e248. doi: 10.1016/j.jacc.2017.11.006. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
