

Alveolar, Endothelial, and Organ Injury Marker Dynamics in Severe COVID-19
- PMID: 34878969
- PMCID: PMC8906476
- DOI: 10.1164/rccm.202106-1514OC
Alveolar, Endothelial, and Organ Injury Marker Dynamics in Severe COVID-19
Abstract
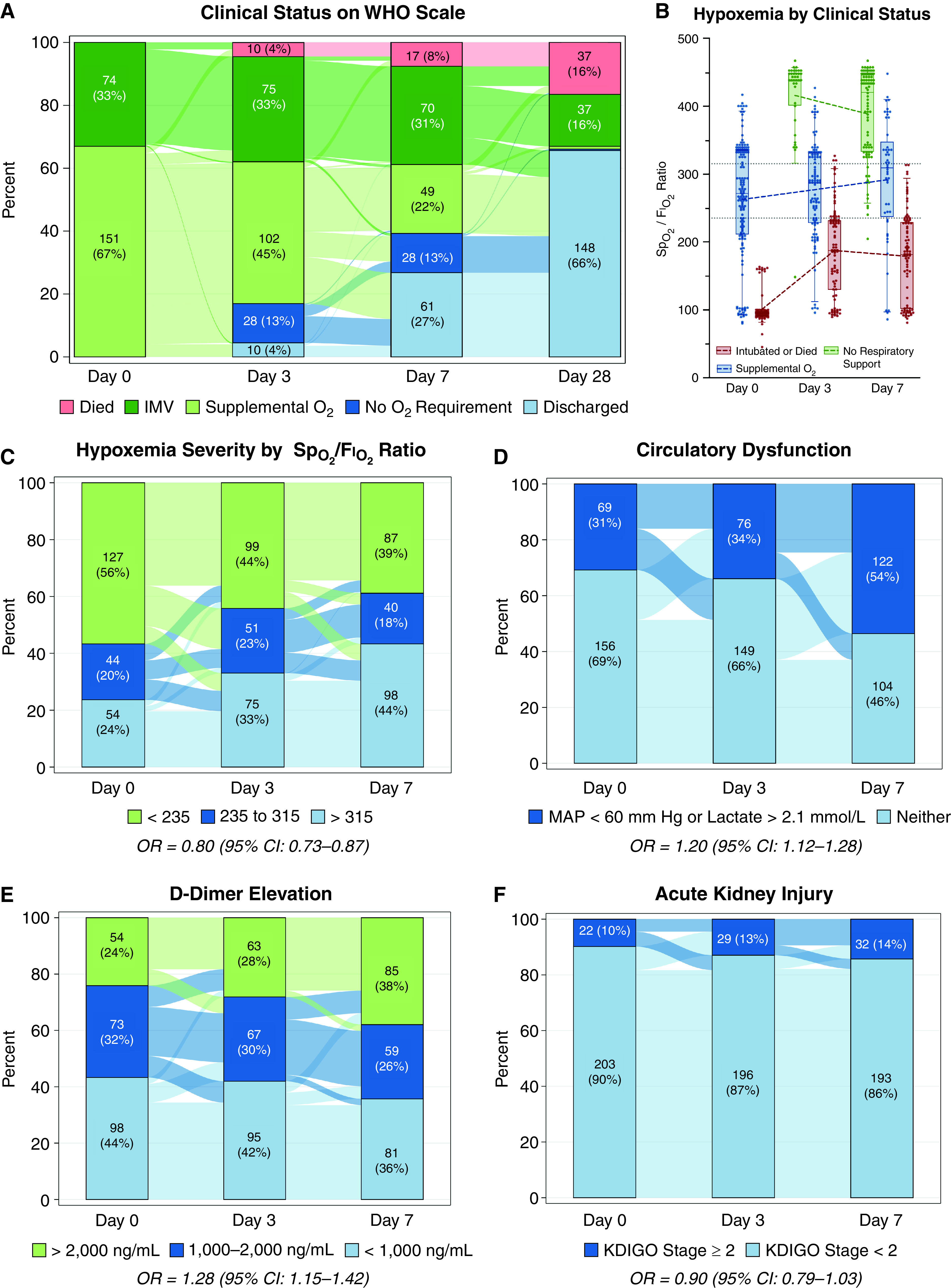
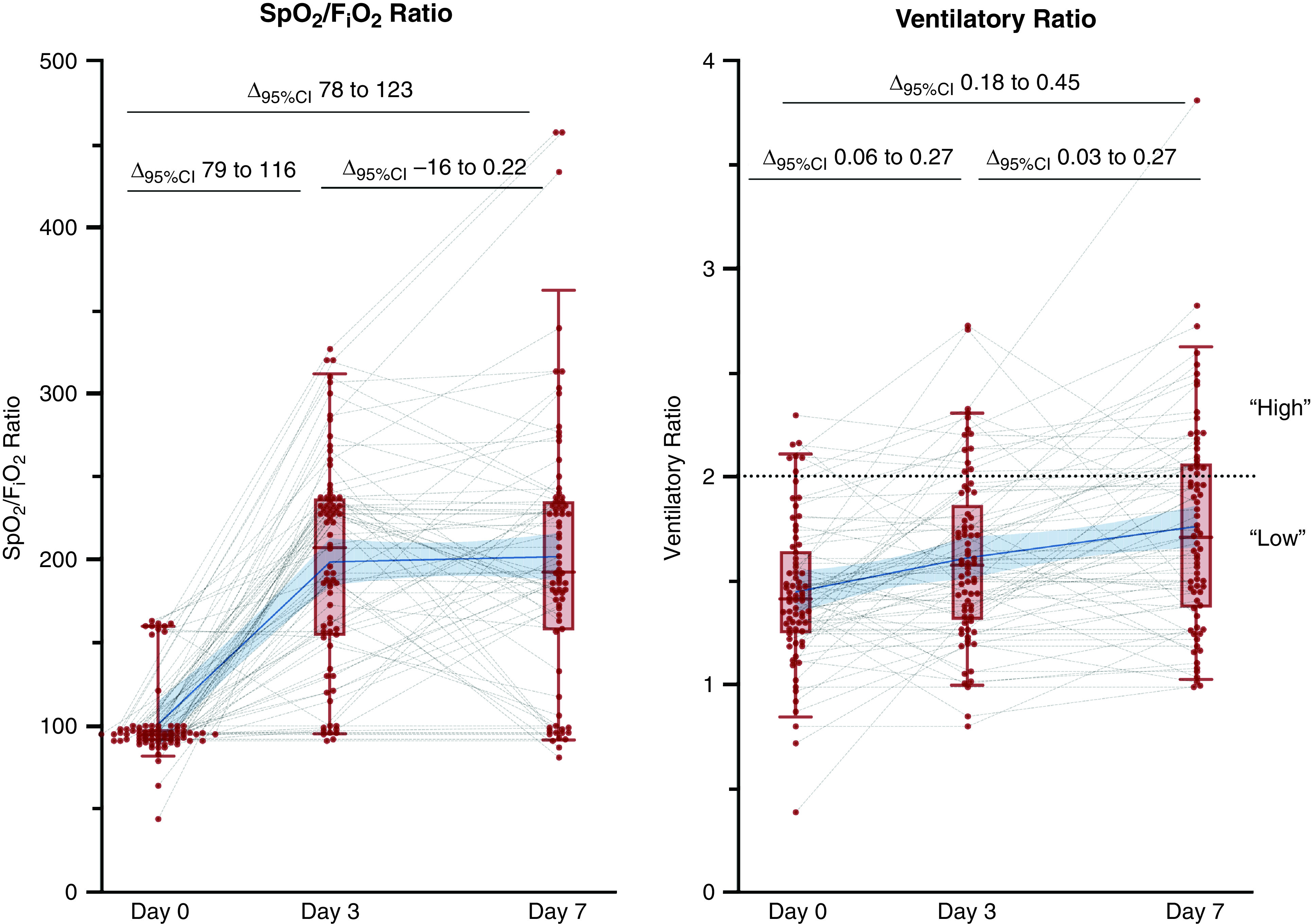
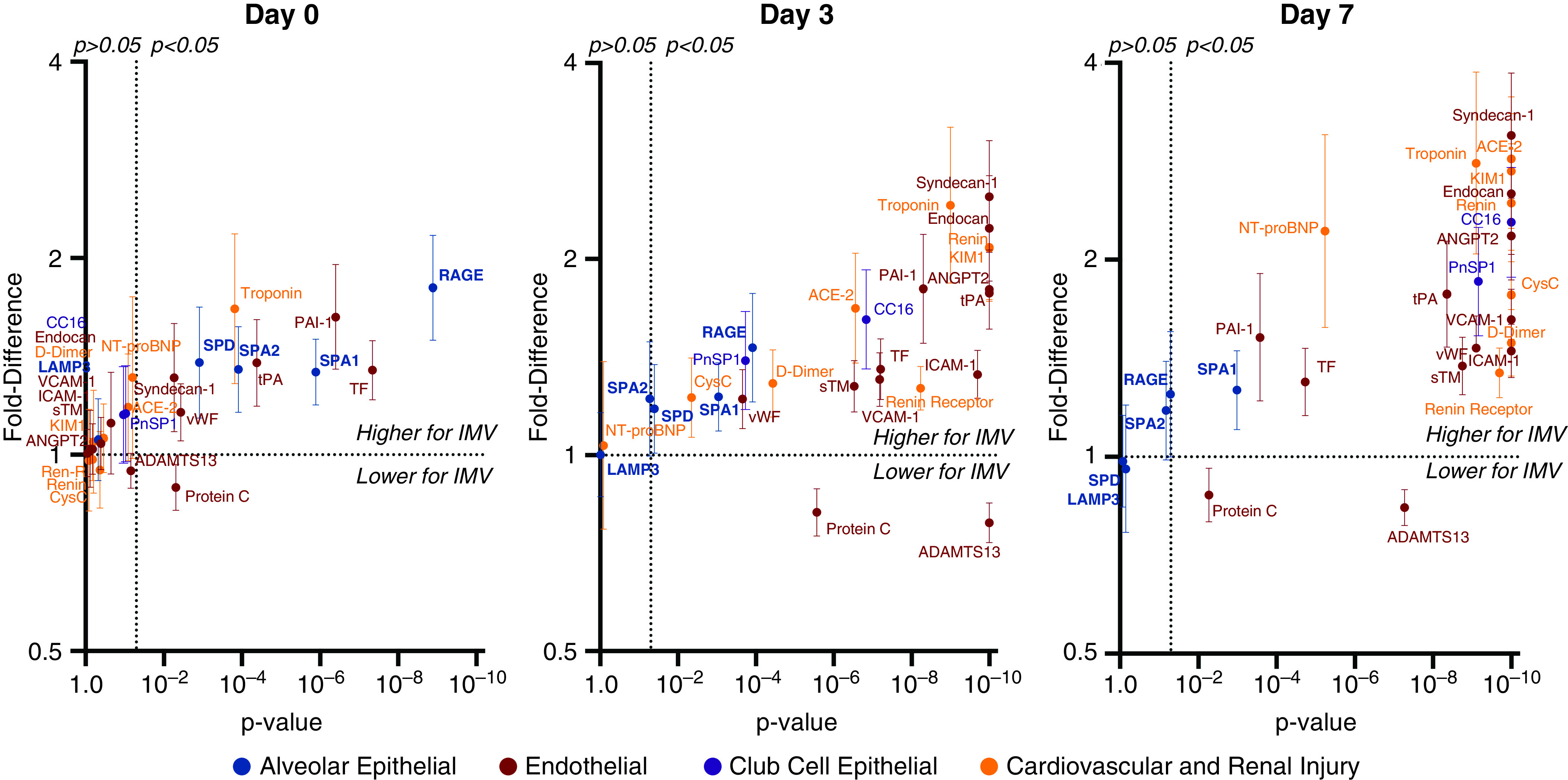
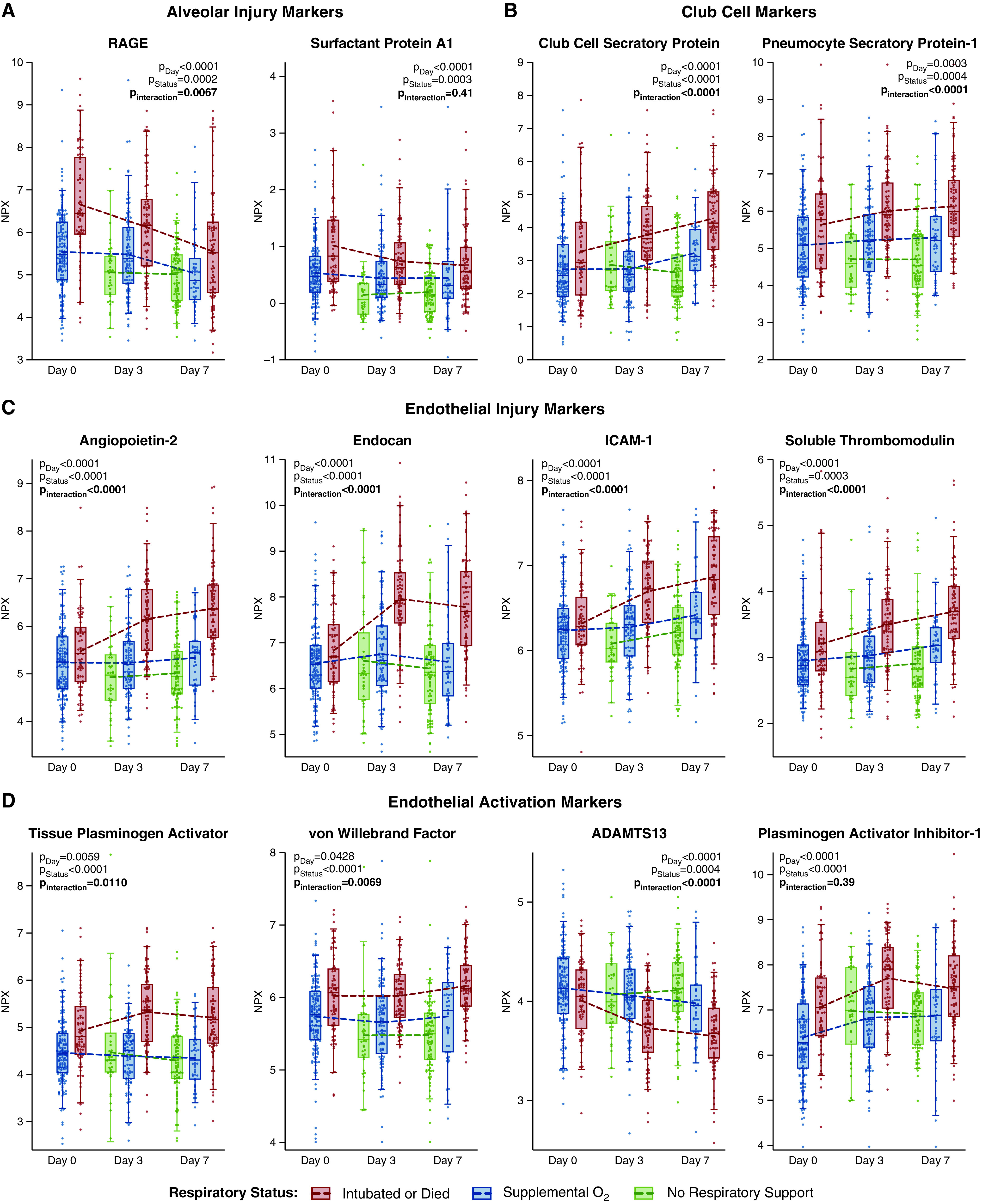
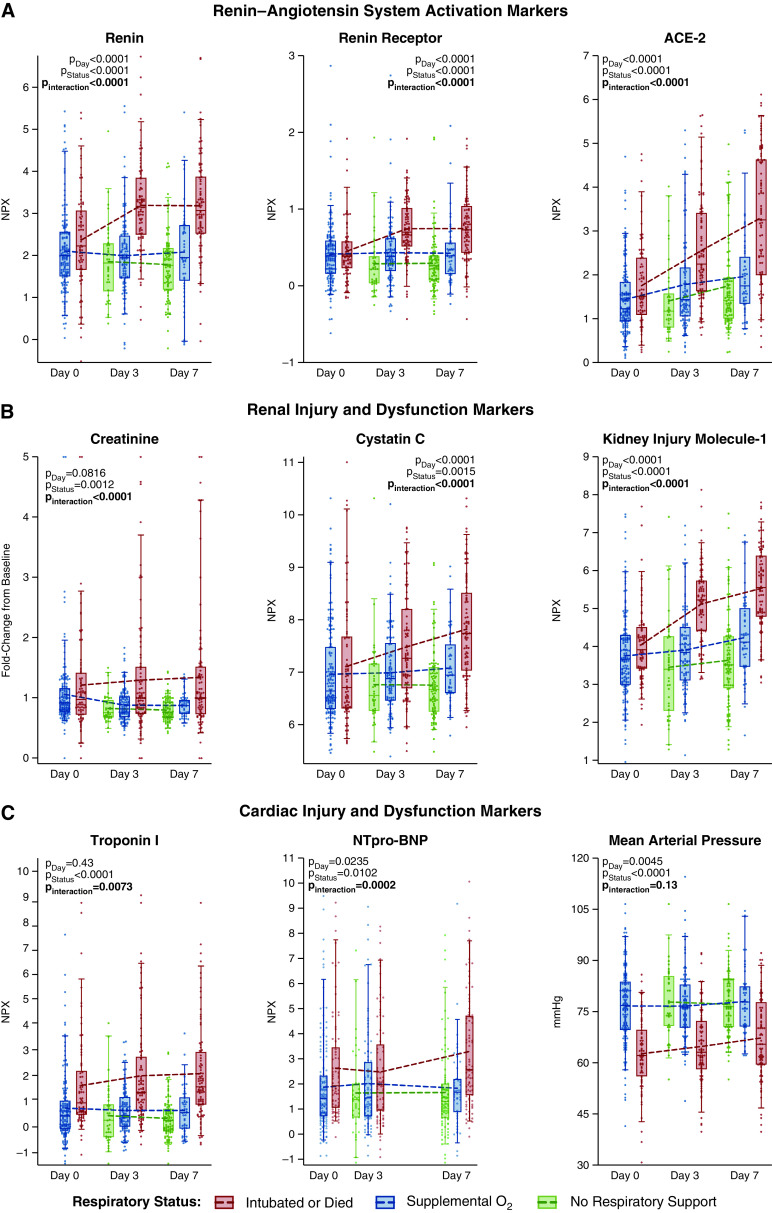
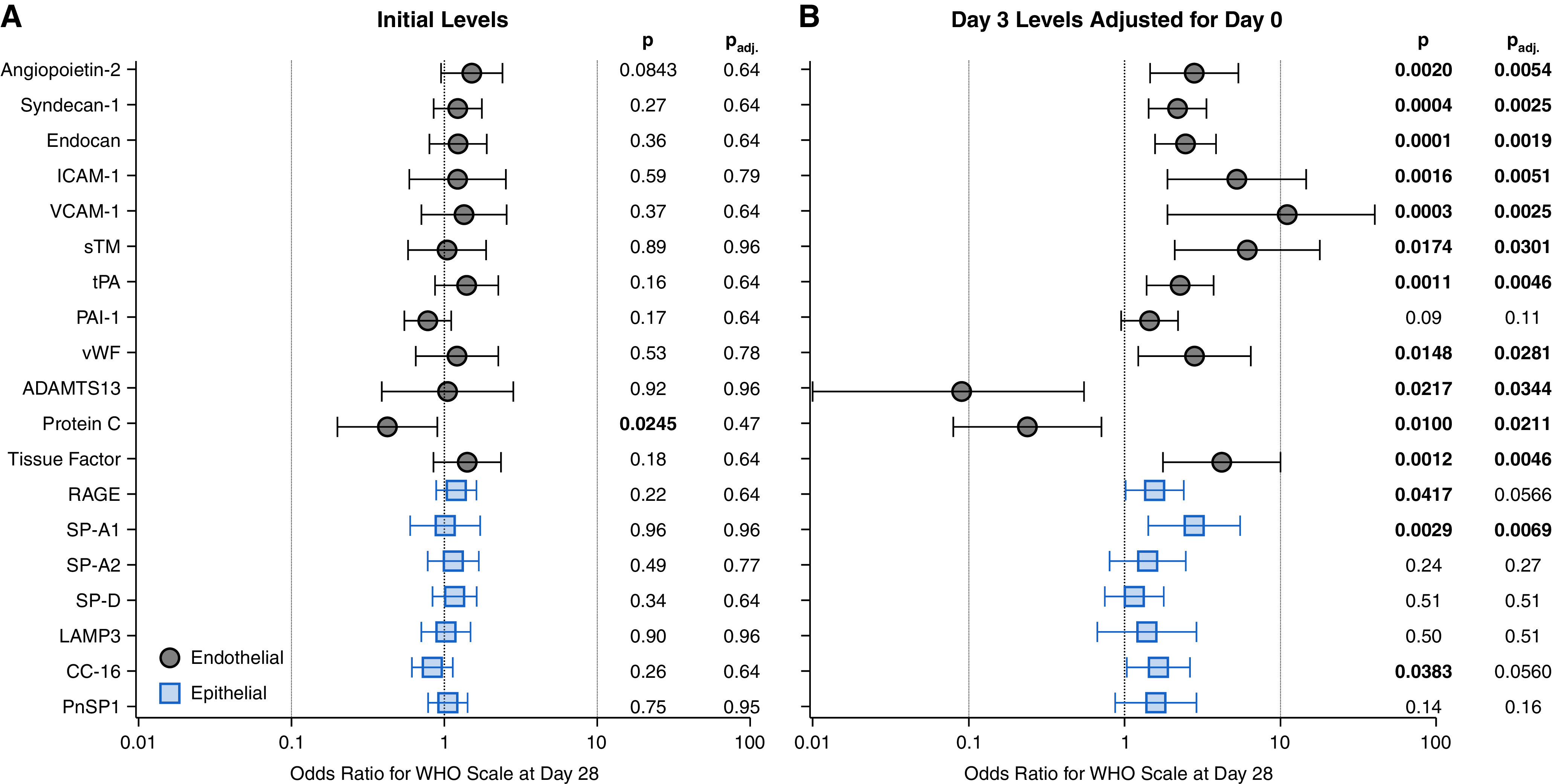
Rationale: Alveolar and endothelial injury may be differentially associated with coronavirus disease (COVID-19) severity over time. Objectives: To describe alveolar and endothelial injury dynamics and associations with COVID-19 severity, cardiorenovascular injury, and outcomes. Methods: This single-center observational study enrolled patients with COVID-19 requiring respiratory support at emergency department presentation. More than 40 markers of alveolar (including receptor for advanced glycation endproducts [RAGE]), endothelial (including angiopoietin-2), and cardiorenovascular injury (including renin, kidney injury molecule-1, and troponin-I) were serially compared between invasively and spontaneously ventilated patients using mixed-effects repeated-measures models. Ventilatory ratios were calculated for intubated patients. Associations of biomarkers with modified World Health Organization scale at Day 28 were determined with multivariable proportional-odds regression. Measurements and Main Results: Of 225 patients, 74 (33%) received invasive ventilation at Day 0. RAGE was 1.80-fold higher in invasive ventilation patients at Day 0 (95% confidence interval [CI], 1.50-2.17) versus spontaneous ventilation, but decreased over time in all patients. Changes in alveolar markers did not correlate with changes in endothelial, cardiac, or renal injury markers. In contrast, endothelial markers were similar to lower at Day 0 for invasive ventilation versus spontaneous ventilation, but then increased over time only among intubated patients. In intubated patients, angiopoietin-2 was similar (fold difference, 1.02; 95% CI, 0.89-1.17) to nonintubated patients at Day 0 but 1.80-fold higher (95% CI, 1.56-2.06) at Day 3; cardiorenovascular injury markers showed similar patterns. Endothelial markers were not consistently associated with ventilatory ratios. Endothelial markers were more often significantly associated with 28-day outcomes than alveolar markers. Conclusions: Alveolar injury markers increase early. Endothelial injury markers increase later and are associated with cardiorenovascular injury and 28-day outcome. Alveolar and endothelial injury likely contribute at different times to disease progression in severe COVID-19.
Keywords: COVID-19; alveolar epithelial cells; endothelium; renin-angiotensin system; respiratory distress syndrome.
Figures
Comment in
-
COVID-19 Pathophysiology: An Opportunity to Start Appreciating Time-Dependent Variation.Am J Respir Crit Care Med. 2022 Mar 1;205(5):483-485. doi: 10.1164/rccm.202112-2857ED. Am J Respir Crit Care Med. 2022. PMID: 35073497 Free PMC article. No abstract available.
-
Reply to Akin et al.: High Renin Concentrations in Severe COVID-19 Are Indicative for a Hypo-Renin-Angiotensin-System State.Am J Respir Crit Care Med. 2022 May 15;205(10):1253-1254. doi: 10.1164/rccm.202202-0292LE. Am J Respir Crit Care Med. 2022. PMID: 35348420 Free PMC article. No abstract available.
-
High Renin Concentrations in Severe COVID-19 Are Indicative for a Hypo-Renin-Angiotensin-System State.Am J Respir Crit Care Med. 2022 May 15;205(10):1252-1253. doi: 10.1164/rccm.202112-2781LE. Am J Respir Crit Care Med. 2022. PMID: 35348428 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
