

A comparison of three strategies to reduce the burden of osteoarthritis: A population-based microsimulation study
- PMID: 34879102
- PMCID: PMC8654220
- DOI: 10.1371/journal.pone.0261017
A comparison of three strategies to reduce the burden of osteoarthritis: A population-based microsimulation study
Abstract
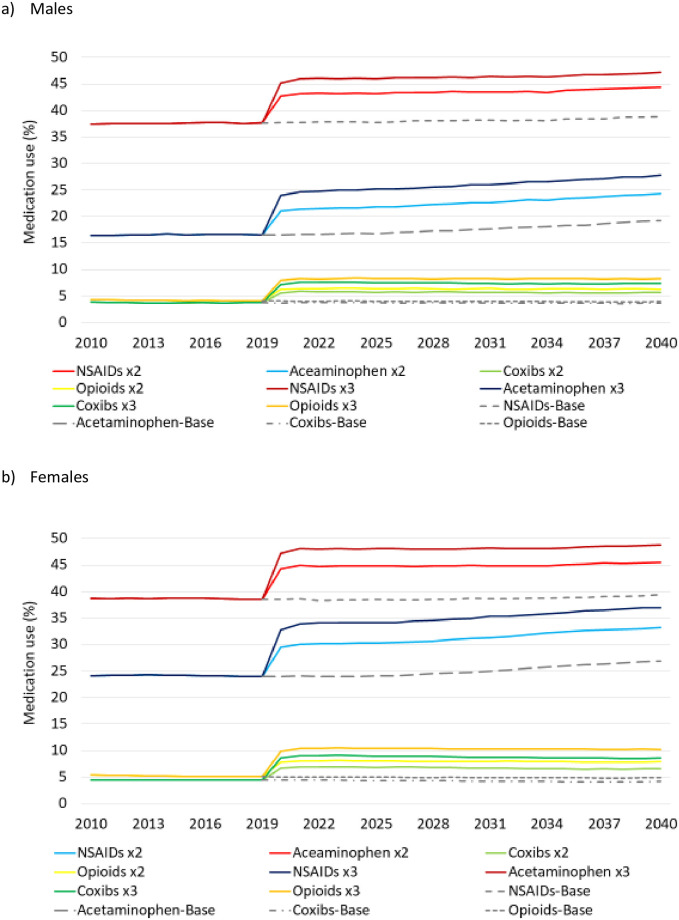
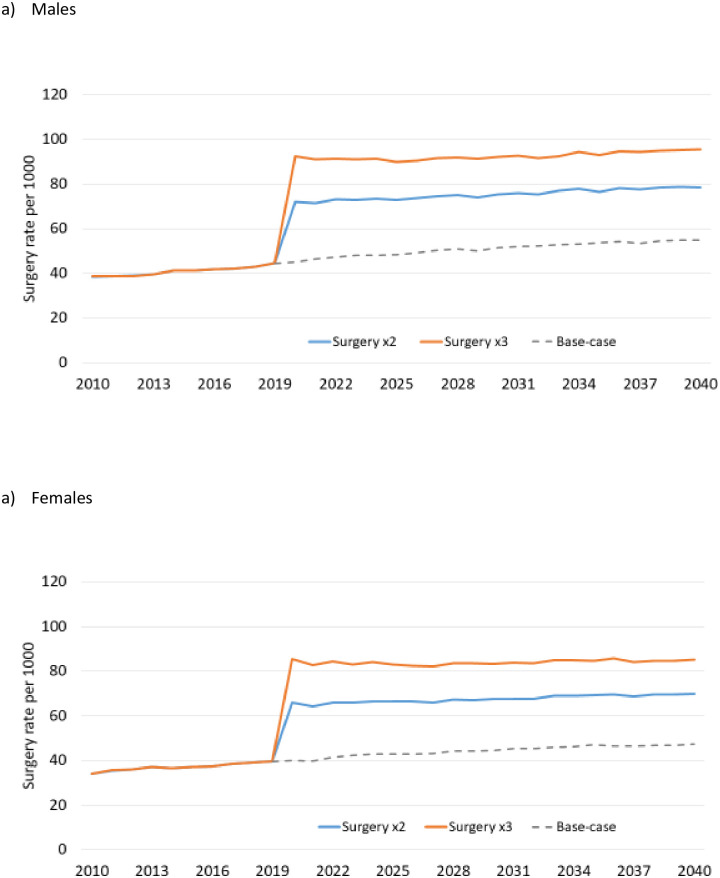
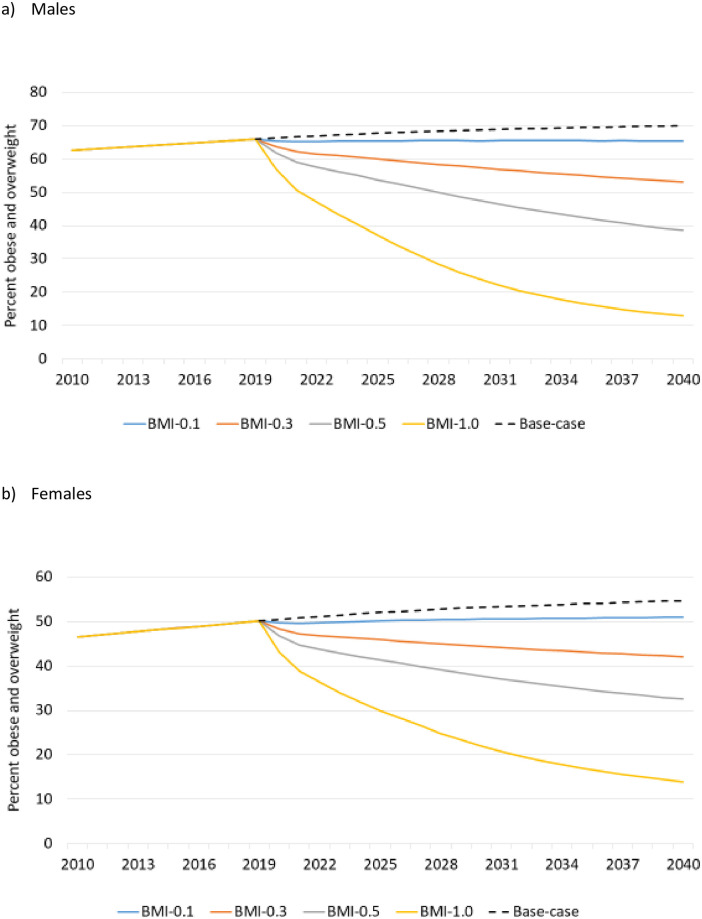
Objectives: The purpose of this study was to compare three strategies for reducing population health burden of osteoarthritis (OA): improved pharmacological treatment of OA-related pain, improved access to joint replacement surgery, and prevention of OA by reducing obesity and overweight.
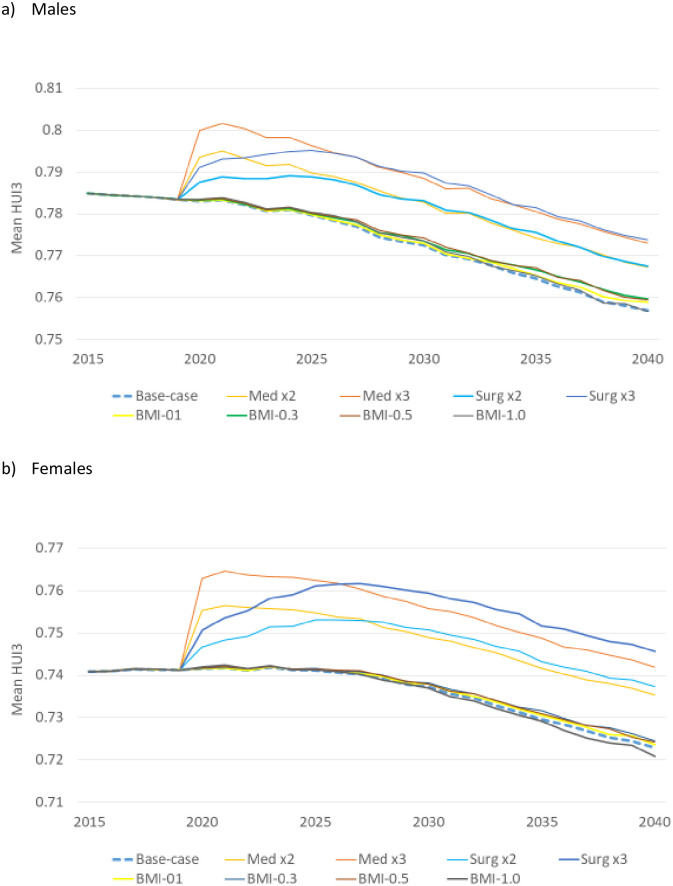
Methods: We applied a validated computer microsimulation model of OA in Canada. The model simulated a Canadian-representative open population aged 20 years and older. Variables in the model included demographics, body mass index, OA diagnosis, OA treatment, mortality, and health-related quality of life. Model parameters were derived from analyses of national surveys, population-based administrative data, a hospital-based cohort study, and the literature. We compared 8 what-if intervention scenarios in terms of disability-adjusted life years (DALYs) relative to base-case, over a wide range of time horizons.
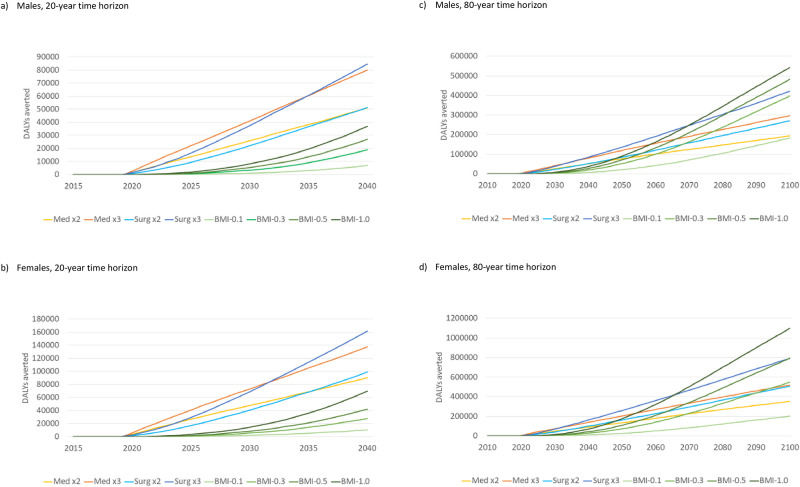
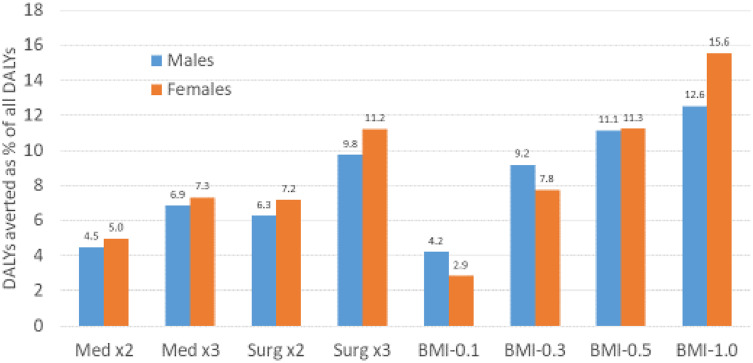
Results: Reductions in DALYs depended on the type of intervention, magnitude of the intervention, and the time horizon. Medical interventions (a targeted increase in the use of painkillers) tended to produce effects quickly and were, therefore, most effective over a short time horizon (a decade). Surgical interventions (increased access to joint replacement) were most effective over a medium time horizon (two decades or longer). Preventive interventions required a substantial change in BMI to generate a significant impact, but produced more reduction in DALYs than treatment strategies over a very long time horizon (several decades).
Conclusions: In this population-based modeling study we assessed the potential impact of three different burden reduction strategies in OA. Data generated by our model may help inform the implementation of strategies to reduce the burden of OA in Canada and elsewhere.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kopec JA, Rahman MM, Berthelot J-M, Le Petit C, Aghajanian J, Sayre EC et al. Descriptive epidemiology of osteoarthritis in British Columbia, Canada. J Rheumatol 2007;34(2):386–93 - PubMed
-
- Global Burden of Disease; Institute of Health Metrix and Evaluation. GBD Compare website. https://vizhub.healthdata.org/gbd-compare/. Accessed: October 7, 2020.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
