

Identifying youth at high risk for sexually transmitted infections in community-based settings using a risk prediction tool: a validation study
- PMID: 34879820
- PMCID: PMC8653586
- DOI: 10.1186/s12879-021-06937-4
Identifying youth at high risk for sexually transmitted infections in community-based settings using a risk prediction tool: a validation study
Abstract
BACKGROUND : Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG) are the most common bacterial sexually transmitted infections (STIs) worldwide. In the absence of affordable point-of-care STI tests, WHO recommends STI testing based on risk factors. This study aimed to develop a prediction tool with a sensitivity of > 90% and efficiency (defined as the percentage of individuals that are eligible for diagnostic testing) of < 60%.
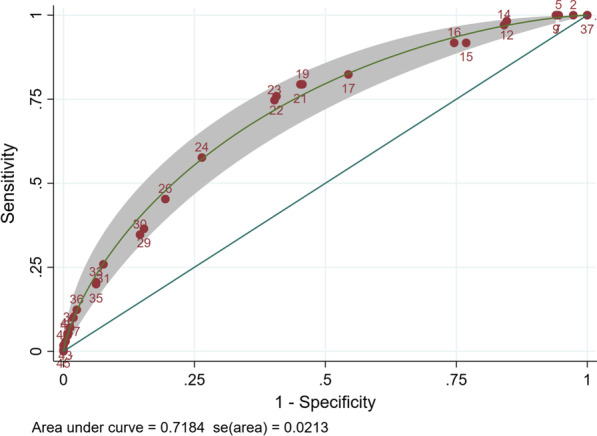
Methods: This study offered CT/NG testing as part of a cluster-randomised trial of community-based delivery of sexual and reproductive health services to youth aged 16-24 years in Zimbabwe. All individuals accepting STI testing completed an STI risk factor questionnaire. The outcome was positivity for either CT or NG. Backwards-stepwise logistic regression was performed with p ≥ 0.05 as criteria for exclusion. Coefficients of variables included in the final multivariable model were multiplied by 10 to generate weights for a STI risk prediction tool. A maximum likelihood Receiver Operating Characteristics (ROC) model was fitted, with the continuous variable score divided into 15 categories of equal size. Sensitivity, efficiency and number needed to screen were calculated for different cut-points.
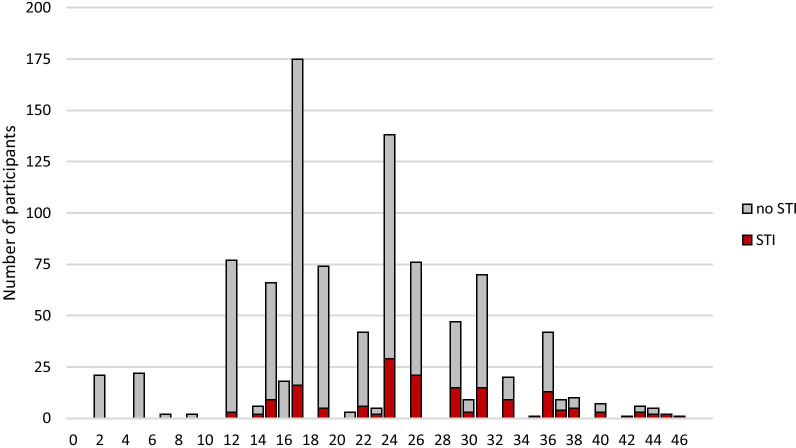
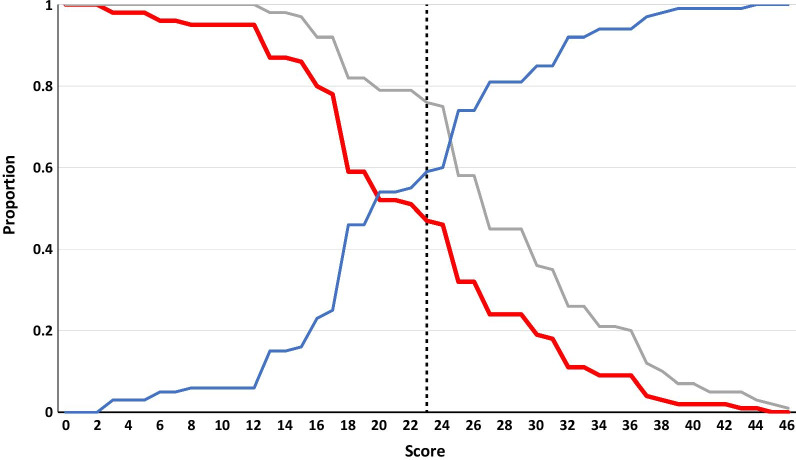
Results: From 3 December 2019 to 5 February 2020, 1007 individuals opted for STI testing, of whom 1003 (99.6%) completed the questionnaire. CT/NG prevalence was 17.5% (95% CI 15.1, 19.8) (n = 175). CT/NG positivity was independently associated with being female, number of lifetime sexual partners, relationship status, HIV status, self-assessed STI risk and past or current pregnancy. The STI risk prediction score including those variables ranged from 2 to 46 with an area under the ROC curve of 0.72 (95% CI 0.68, 0.76). Two cut-points were chosen: (i) 23 for optimised sensitivity (75.9%) and specificity (59.3%) and (ii) 19 to maximise sensitivity (82.4%) while keeping efficiency at < 60% (59.4%).
Conclusions: The high prevalence of STIs among youth, even in those with no or one reported risk factor, may preclude the use of risk prediction tools for selective STI testing. At a cut-point of 19 one in six young people with STIs would be missed.
Keywords: Adolescents; Risk prediction tool; Screening; Sexually transmitted infections.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
