

Ischemic Stroke and Pulmonary Arteriovenous Malformations: A Review
- PMID: 34880092
- PMCID: PMC8826462
- DOI: 10.1212/WNL.0000000000013169
Ischemic Stroke and Pulmonary Arteriovenous Malformations: A Review
Erratum in
-
Ischemic Stroke and Pulmonary Arteriovenous Malformations: A Review.Neurology. 2022 May 17;98(20):864. doi: 10.1212/WNL.0000000000200275. Epub 2022 Mar 2. Neurology. 2022. PMID: 35236773 Free PMC article. No abstract available.
Abstract
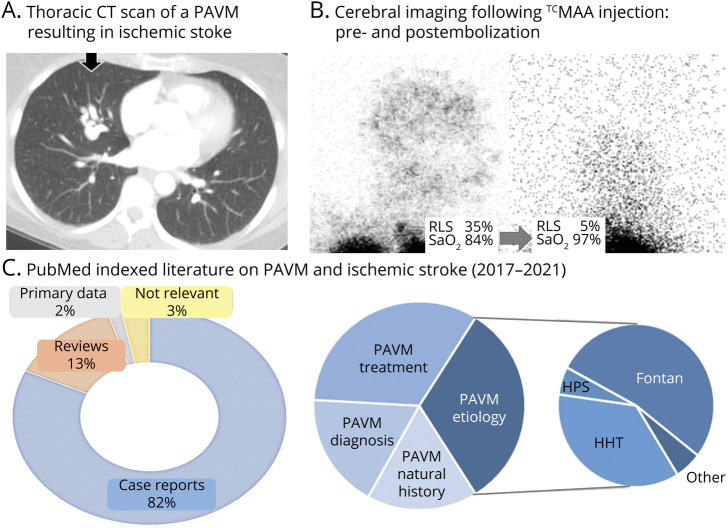
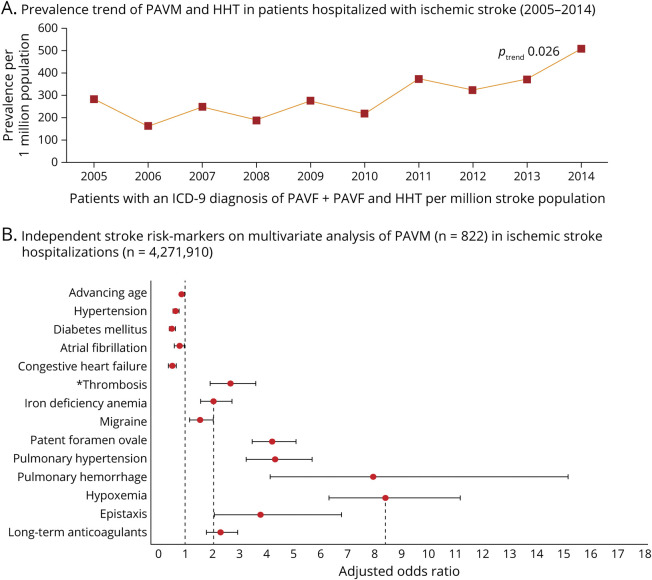
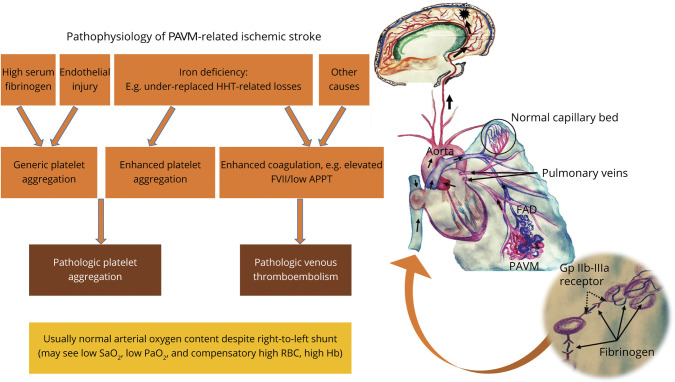
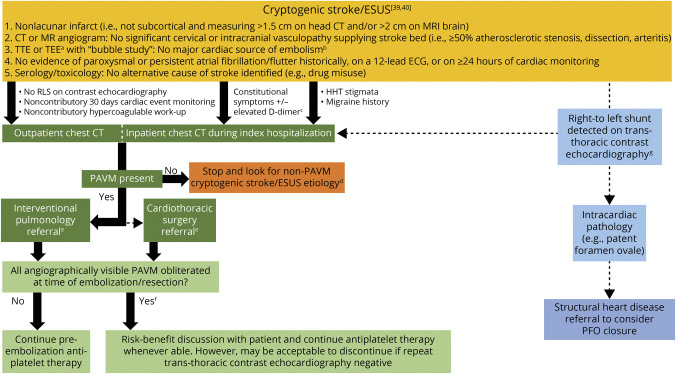
The potential of covert pulmonary arteriovenous malformations (PAVMs) to cause early onset, preventable ischemic strokes is not well known to neurologists. This is evident by their lack of mention in serial American Heart Association/American Stroke Association (AHA/ASA) Guidelines and the single case report biased literature of recent years. We performed PubMed and Cochrane database searches for major studies on ischemic stroke and PAVMs published from January 1, 1974, through April 3, 2021. This identified 24 major observational studies, 3 societal guidelines, 1 nationwide analysis, 3 systematic reviews, 21 other review/opinion articles, and 18 recent (2017-2021) case reports/series that were synthesized. Key points are that patients with PAVMs have ischemic stroke a decade earlier than routine stroke, losing 9 extra healthy life-years per patient in the recent US nationwide analysis (2005-2014). Large-scale thoracic CT screens of the general population in Japan estimate PAVM prevalence to be 38/100,000 (95% confidence interval 18-76), with ischemic stroke rates exceeding 10% across PAVM series dating back to the 1950s, with most PAVMs remaining undiagnosed until the time of clinical stroke. Notably, the rate of PAVM diagnoses doubled in US ischemic stroke hospitalizations between 2005 and 2014. The burden of silent cerebral infarction approximates to twice that of clinical stroke. More than 80% of patients have underlying hereditary hemorrhagic telangiectasia. The predominant stroke mechanism is paradoxical embolization of platelet-rich emboli, with iron deficiency emerging as a modifiable risk factor. PAVM-related ischemic strokes may be cortical or subcortical, but very rarely cause proximal large vessel occlusions. Single antiplatelet therapy may be effective for secondary stroke prophylaxis, with dual antiplatelet or anticoagulation therapy requiring nuanced risk-benefit analysis given their risk of aggravating iron deficiency. This review summarizes the ischemic stroke burden from PAVMs, the implicative pathophysiology, and relevant diagnostic and treatment overviews to facilitate future incorporation into AHA/ASA guidelines.
© 2021 American Academy of Neurology.
Figures
References
-
- Shovlin CL, Condliffe R, Donaldson JW, Kiely DG, Wort SJ, British Thoracic Society. British Thoracic Society clinical statement on pulmonary arteriovenous malformations. Thorax. 2017;72(12):1154-1163. - PubMed