

Passive detection of COVID-19 with wearable sensors and explainable machine learning algorithms
- PMID: 34880366
- PMCID: PMC8655005
- DOI: 10.1038/s41746-021-00533-1
Passive detection of COVID-19 with wearable sensors and explainable machine learning algorithms
Abstract
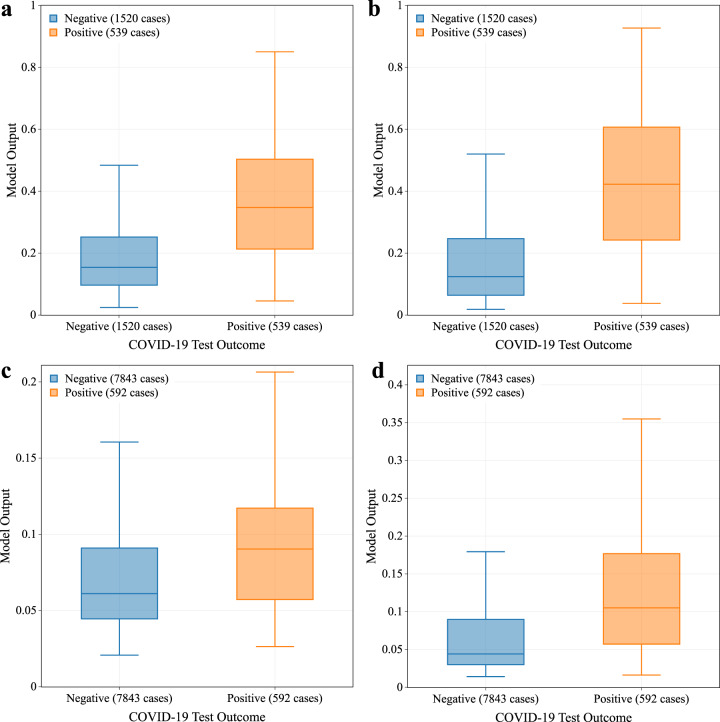
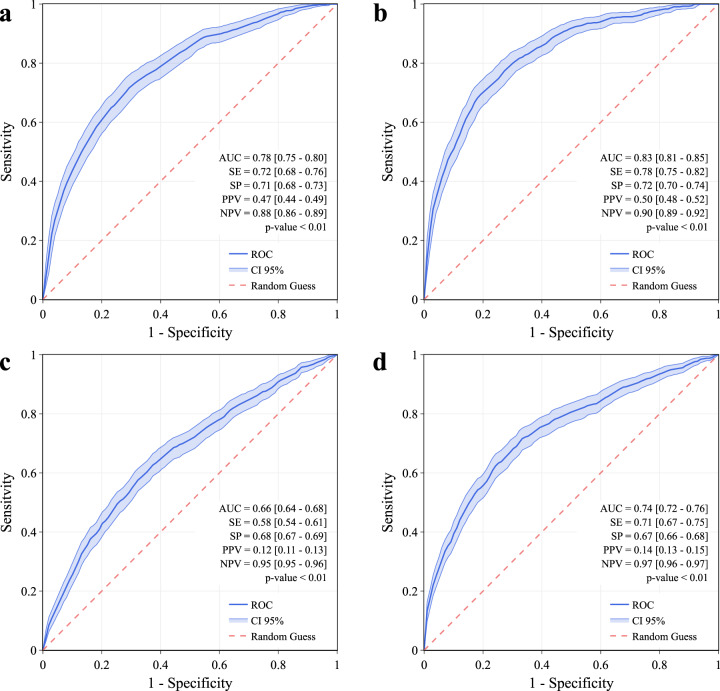
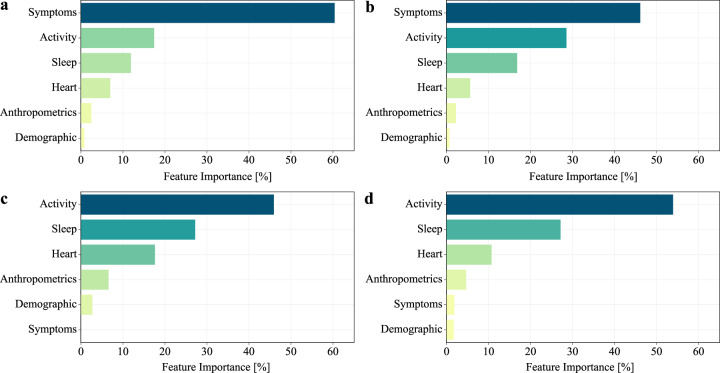
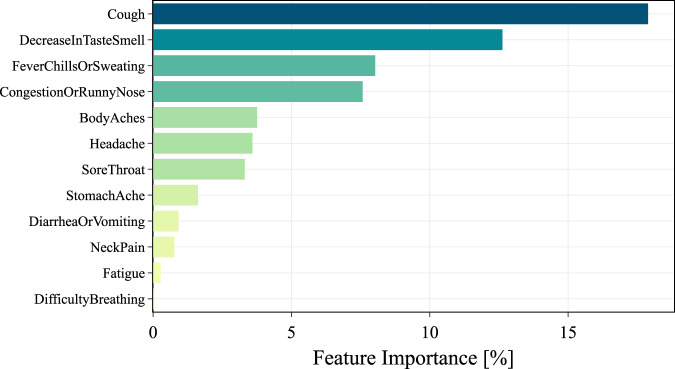
Individual smartwatch or fitness band sensor data in the setting of COVID-19 has shown promise to identify symptomatic and pre-symptomatic infection or the need for hospitalization, correlations between peripheral temperature and self-reported fever, and an association between changes in heart-rate-variability and infection. In our study, a total of 38,911 individuals (61% female, 15% over 65) have been enrolled between March 25, 2020 and April 3, 2021, with 1118 reported testing positive and 7032 negative for COVID-19 by nasopharyngeal PCR swab test. We propose an explainable gradient boosting prediction model based on decision trees for the detection of COVID-19 infection that can adapt to the absence of self-reported symptoms and to the available sensor data, and that can explain the importance of each feature and the post-test-behavior for the individuals. We tested it in a cohort of symptomatic individuals who exhibited an AUC of 0.83 [0.81-0.85], or AUC = 0.78 [0.75-0.80] when considering only data before the test date, outperforming state-of-the-art algorithm in these conditions. The analysis of all individuals (including asymptomatic and pre-symptomatic) when self-reported symptoms were excluded provided an AUC of 0.78 [0.76-0.79], or AUC of 0.70 [0.69-0.72] when considering only data before the test date. Extending the use of predictive algorithms for detection of COVID-19 infection based only on passively monitored data from any device, we showed that it is possible to scale up this platform and apply the algorithm in other settings where self-reported symptoms can not be collected.
© 2021. The Author(s).
Conflict of interest statement
S.R.S. is employed by PhysIQ. The other authors declare no competing interests.
Figures

References
-
- NIH. COVID-19 Treatment Guidelines. https://www.covid19treatmentguidelines.nih.gov/whats-new/ (NIH, 2021).
-
- Quer G, Gouda P, Galarnyk M, Topol EJ, Steinhubl SR. Inter- and intraindividual variability in daily resting heart rate and its associations with age, sex, sleep, BMI, and time of year: Retrospective, longitudinal cohort study of 92,457 adults. PLoS ONE. 2020;15:e0227709. doi: 10.1371/journal.pone.0227709. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
