

Health-Care Utilization and Outcomes with 10 kHz Spinal Cord Stimulation for Chronic Refractory Pain
- PMID: 34880672
- PMCID: PMC8648088
- DOI: 10.2147/JPR.S306126
Health-Care Utilization and Outcomes with 10 kHz Spinal Cord Stimulation for Chronic Refractory Pain
Abstract
Background: Chronic pain is a common condition associated with decreased quality of life and increased health-care costs. Opioid analgesics are routinely used to treat chronic pain despite limited evidence of long-term efficacy. Spinal cord stimulation at a frequency of 10 kilohertz (10kHz-SCS) has been shown to be effective for treating chronic pain.
Objective: This study was conducted to evaluate the effects of 10kHz-SCS on patients' pain intensity, volume of pain interventions, and opioid intake in a real-world setting.
Study design: This study was a retrospective review of patient data.
Setting: The study was conducted at a single, community-based clinic.
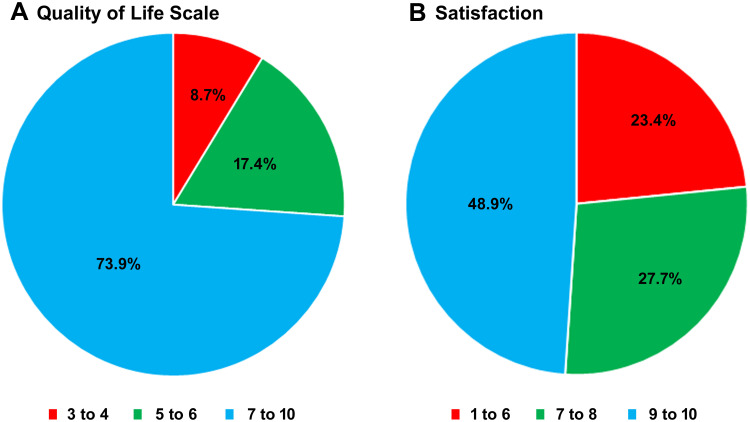
Methods: Outcomes including pain relief, quality of life, opioid intake, and rate of health-care usage were evaluated using data from patients who were implanted with a 10kHz-SCS device to treat chronic pain. These outcomes were then compared for the pre- and post-implant periods.
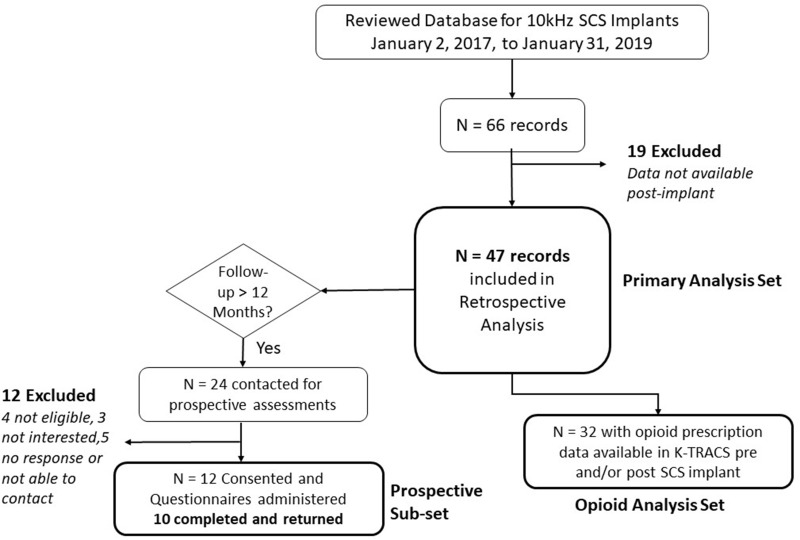
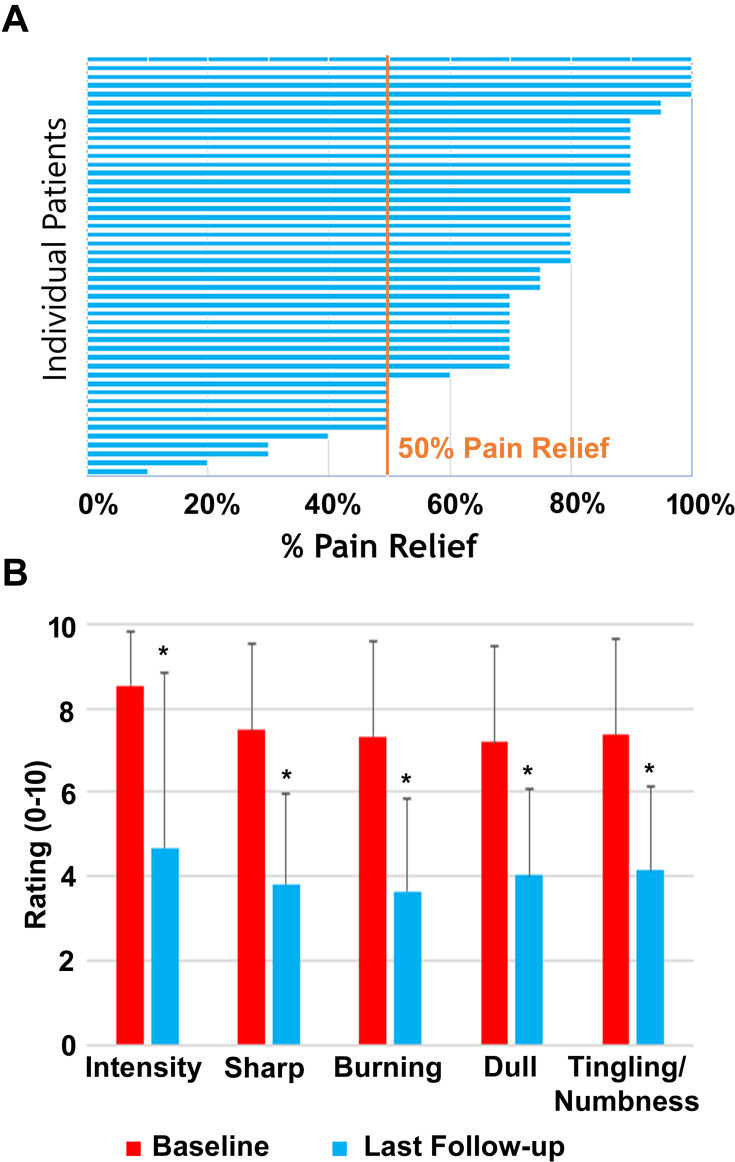
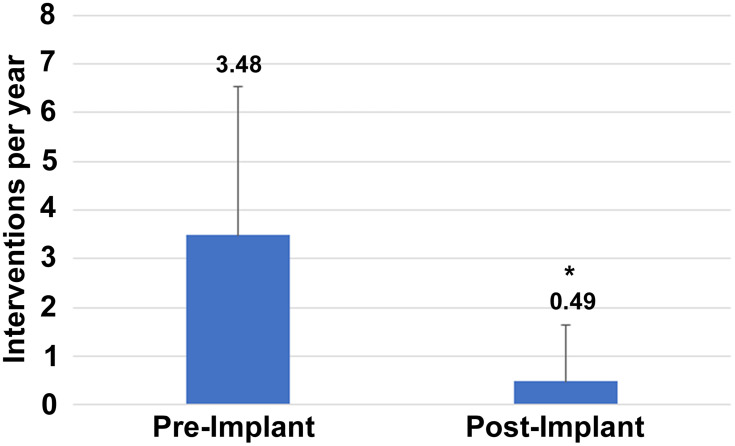
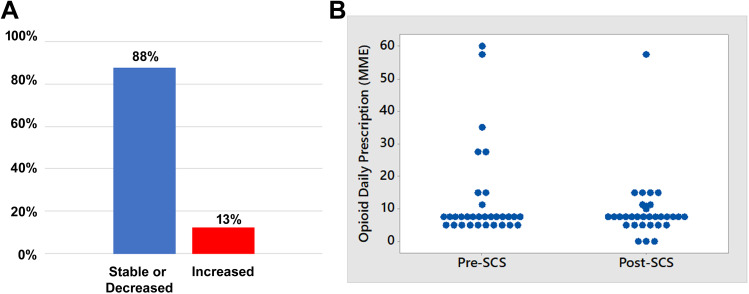
Results: A total of 47 patients with a mean follow-up duration of 15.6 ± 6.2 months were included in this analysis. Mean pain relief was 73 ± 22% and 89% were responders at the final follow-up visit. The rate of medical interventions fell from 3.48±3.05 per year before starting 10kHz-SCS to 0.49±1.16 per year afterward (P < 0.001). Of 30 patients with available opioid consumption data, 89% maintained or decreased their intake after implant.
Conclusion: Retrospective data from a single center, with minimal exclusion criteria shows clinically significant pain relief with 10kHz-SCS, accompanied by significant indirect benefits including stable or reduced opioid use and reduced interventional procedures.
Keywords: chronic pain; health care costs; opioid analgesics; pain management; spinal cord stimulation.
© 2021 Gupta et al.
Conflict of interest statement
This study was supported by an unrestricted grant from Nevro Corp. Dr. Mayank Gupta reports grants from Nevro Corp., during the conduct of the study; personal fees from Nevro Corp., outside the submitted work; Consultant-Self Advisory/Medical Board-Self Investigator-Self from Averitas Pharma, Consultant-Self Investigator-Self from US WorldMeds, Consultant-Self Investigator-Self from Nalu Medical, Consultant-Self Advisory/Medical Board-Self from Foundation Fusion Solutions, Consultant-Self Investigator-Self from SPR Therapeutics, Inc., during the conduct of the study. The authors report no other conflicts of interest in this work.
Figures
References
-
- Institute of Medicine. Relieving pain in America: A blueprint for transforming prevention, care, education, and research. Washington, DC: The National Academies Press; 2011. - PubMed
-
- Schappert SM, Burt CW. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001-02. Vital Health Stat. 2006;13(159):1–66. - PubMed
LinkOut - more resources
Full Text Sources
