

Scaphotrapezoid Assessment during Thumb Carpometacarpal Arthroplasty: A Cadaveric Study
- PMID: 34881109
- PMCID: PMC8635814
- DOI: 10.1055/s-0041-1729992
Scaphotrapezoid Assessment during Thumb Carpometacarpal Arthroplasty: A Cadaveric Study
Abstract
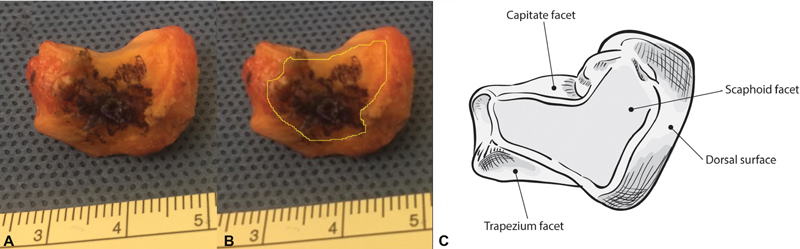
Background Due to limited sensitivity of radiographs for scaphotrapeziotrapezoid (STT) arthritis and the high rate of concurrence between thumb carpometacarpal (CMC) and STT arthritis, intraoperative visualization of the STT joint is recommended during CMC arthroplasty. Purpose We quantified the percentage of trapezoid facet of the scaphotrapezoid (ST) joint that could be visualized during this approach, and compared it to the degree of preoperative radiographic STT arthritis. Methods We performed dorsal surgical approach to the thumb CMC joint after obtaining fluoroscopic anteroposterior, lateral, and oblique wrist radiographs of 11 cadaver wrists. After trapeziectomy, the ST joint was inspected and the visualized portion of the trapezoid articulation marked with an electrocautery. The trapezoid was removed, photographed, and the marked articular surface area and total surface area were independently measured by two authors using an image analysis software. The radiographs were analyzed for the presence of STT arthritis. Results The mean visualized trapezoid surface area during standard approach for CMC arthroplasty was 60.3% (standard deviation: 24.6%). The visualized percentage ranged widely from 16.7 to 96.5%. There was no significant correlation between degree of radiographic arthritis and visualized percentage of the joint ( p = 0.77). Conclusions: On average, 60% of the trapezoid joint surface was visualized during routine approach to the thumb CMC joint, but with very large variability. Direct visualization of the joint did not correlate with the degree of radiographic STT arthritis. Clinical Relevance A combination of clinical examination, pre- and intraoperative radiographs, and intraoperative visualization should be utilized to assess for STT osteoarthritis and determine the need for surgical treatment. Level of Evidence This is a Cadaveric Research Article.
Keywords: CMC; STT; carpometacarpal arthritis; intraoperative visualization; scaphotrapeziotrapezoid arthritis; scaphotrapezoid.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures


References
-
- Haara M M, Heliövaara M, Kröger H. Osteoarthritis in the carpometacarpal joint of the thumb. Prevalence and associations with disability and mortality. J Bone Joint Surg Am. 2004;86(07):1452–1457. - PubMed
-
- Armstrong A L, Hunter J B, Davis T R. The prevalence of degenerative arthritis of the base of the thumb in post-menopausal women. J Hand Surg [Br] 1994;19(03):340–341. - PubMed
-
- Tomaino M M, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am. 1999;24(06):1220–1224. - PubMed
-
- Bhatia A, Pisoh T, Touam C, Oberlin C. Incidence and distribution of scaphotrapezotrapezoidal arthritis in 73 fresh cadaveric wrists. Ann Chir Main Memb Super. 1996;15(04):220–225. - PubMed
