

Meniscal and Cartilage Changes on Serial MRI After Medial Opening-Wedge High Tibial Osteotomy
- PMID: 34881345
- PMCID: PMC8647275
- DOI: 10.1177/23259671211047904
Meniscal and Cartilage Changes on Serial MRI After Medial Opening-Wedge High Tibial Osteotomy
Abstract
Background: Assessments of the effects of realignment using opening-wedge high tibial osteotomy (OWHTO) on the medial, lateral, and patellofemoral compartments have been limited to cartilage evaluations.
Purpose/hypothesis: The purpose was to evaluate the effects of OWHTO on the meniscus and cartilage of each compartment as a cooperative unit (meniscochondral unit) using serial magnetic resonance imaging (MRI). It was hypothesized that (1) favorable changes in the meniscochondral unit would occur in the medial compartment and (2) that changes in the patellofemoral and lateral compartments would be negligible.
Study design: Case series; Level of evidence, 4.
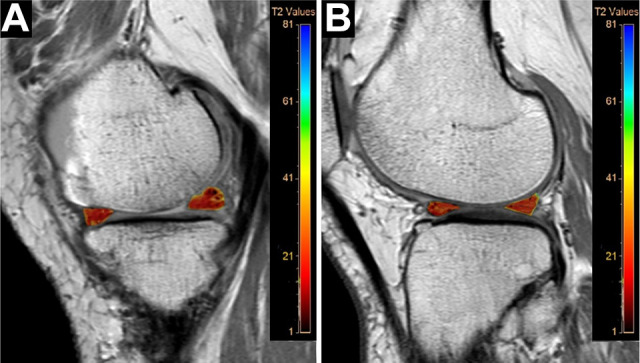
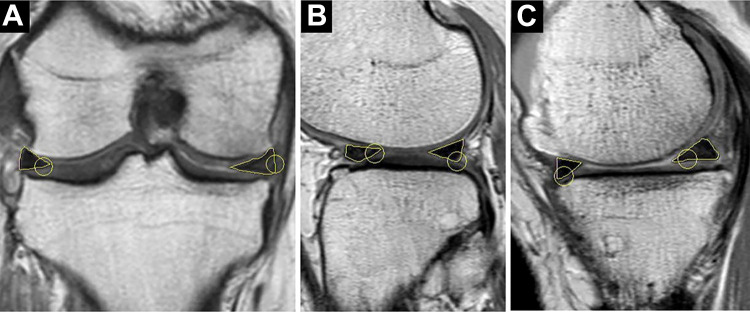
Methods: Included were 36 knees that underwent OWHTO from March 2014 to February 2016 and had postoperative serial MRI. The MRI was performed at 19.9 ± 7.4 and 52.3 ± 8.3 months postoperatively, and the cartilage and meniscal changes were evaluated by highlighting the regions of interest. We evaluated the T2 relaxation times of each cartilage and meniscal area, the cross-sectional area of the menisci, and the extrusion of the medial meniscus (MM). The meniscochondral unit was assessed using subgroup analyses according to the status of the MM.
Results: Significant decreases were seen in T2 relaxation times in the medial femoral condyle (MFC) (P < .001) and medial tibial plateau (MTP) (P = .050), and significant increases were seen in the lateral femoral condyle (LFC) (P = .036). The change was more prominent in the MFC compared with the MTP and LFC (P = .003). No significant changes were observed in the lateral tibial plateau, patella, or trochlear groove. The area of the lateral meniscus (body and posterior horn) was decreased compared with preoperative MRI (P < .001 for both). The extent of MM extrusion decreased between the preoperative, first follow-up, and second follow-up MRIs (P < .001).
Conclusion: OWHTO affected the medial compartment positively, the lateral compartment negatively, and the patellofemoral compartment negligibly. The effects were more prominent and consistent in the medial than in the lateral compartment.
Keywords: T2 relaxation time; cartilage; magnetic resonance imaging; meniscus; opening wedge high tibial osteotomy.
© The Author(s) 2021.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures



References
-
- Adams J, McAlindon T, Dimasi M, Carey J, Eustace S. Contribution of meniscal extrusion and cartilage loss to joint space narrowing in osteoarthritis. Clin Radiol. 1999;54(8):502–506. - PubMed
-
- Biswal S, Hastie T, Andriacchi TP, et al. Risk factors for progressive cartilage loss in the knee: a longitudinal magnetic resonance imaging study in forty-three patients. Arthritis Rheum. 2002;46(11):2884–2892. - PubMed
-
- Buckwalter J, Mankin H. Articular cartilage: degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect. 1998;47:487–504. - PubMed
LinkOut - more resources
Full Text Sources
