

Clinical outcomes, molecular epidemiology and resistance mechanisms of multidrug-resistant Pseudomonas aeruginosa isolated from bloodstream infections from Qatar
- PMID: 34882052
- PMCID: PMC8667892
- DOI: 10.1080/07853890.2021.2012588
Clinical outcomes, molecular epidemiology and resistance mechanisms of multidrug-resistant Pseudomonas aeruginosa isolated from bloodstream infections from Qatar
Abstract
Background: Bloodstream infections (BSIs) caused by multidrug-resistant (MDR)-Pseudomonas aeruginosa are associated with poor clinical outcomes, at least partly due to delayed appropriate antimicrobial therapy. The characteristics of MDR-P. aeruginosa bloodstream isolates have not been evaluated in Qatar. Our study aimed to examine in vitro susceptibility, clinical and molecular characteristics, and mechanisms of resistance of MDR-P. aeruginosa bloodstream isolates from Qatar.
Materials and methods: We included all MDR-P. aeruginosa isolated from blood cultures taken between October 2014 and September 2017. Blood cultures were processed using BD BACTEC™ FX automated system. BD Phoenix™ was used for identification, Liofilchem® MIC Test Strips for MIC determination. Whole-genome sequencing was performed using the Illumina-HiSeq-2000.
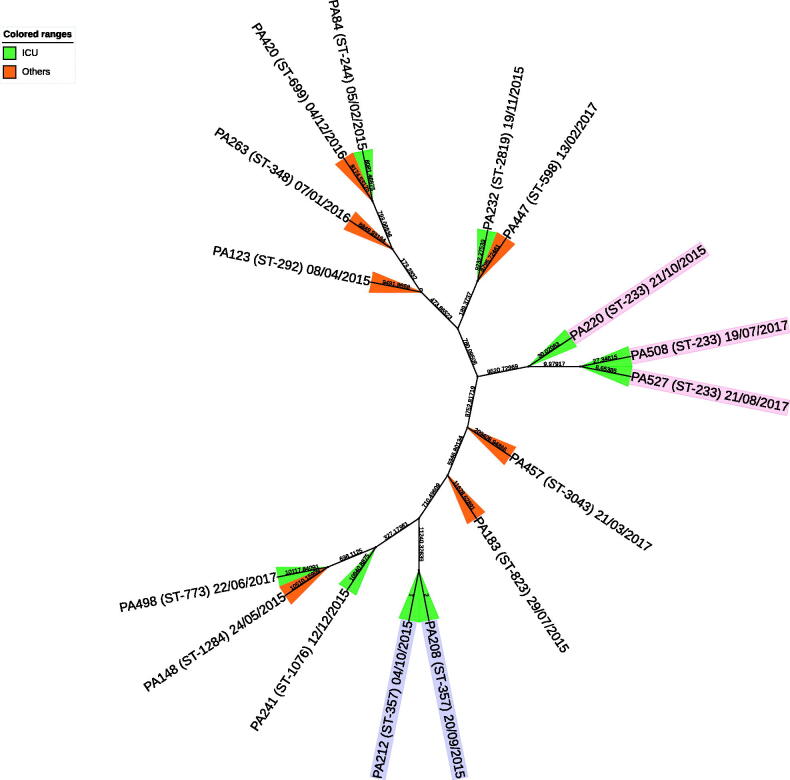
Results: Out of 362 P. aeruginosa bloodstream isolates, 16 (4.4%) were MDR. The median patient age was 55 years (range 43-81) and all patients presented with septic shock. Most patients received meropenem (12/16) and/or colistin (10/16). Clinical response was achieved in eight patients, and five patients died within 30-days. MDR-P. aeruginosa isolates belonged to 13 different sequence types. All isolates were non-susceptible to cefepime and ciprofloxacin. The most active agents were colistin (16/16) and aztreonam (10/16). Seven isolates produced blaVIM, and four possessed genes encoding extended-spectrum β-lactamases. Aminoglycoside modifying enzymes were present in 15/16, transferable qnr-mediated quinolone resistance gene was detected in 3/16, and the novel ciprofloxacin modifying enzyme CrpP-encoding gene in one isolate.
Conclusion: MDR-P. aeruginosa BSIs are relatively uncommon in Qatar but are highly resistant, harbour multiple resistance genes, and are commonly associated with unfavourable clinical outcomes. Colistin was the only agent with consistent activity against the study isolates.Key messagesMDR-P. aeruginosa constituted <5% of P. aeruginosa blood isolates over three years.Typical risk factors for MDR infections were highly prevalent in the study population and overall clinical outcomes are consistent with those previously reported.Colistin was the only agent with consistent antibacterial activity against the study isolates.
Keywords: Bacteraemia; MDR; Pseudomonas aeruginosa; Qatar.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures

References
-
- Tumbarello M, Repetto E, Trecarichi EM, et al. . Multidrug-resistant Pseudomonas aeruginosa bloodstream infections: risk factors and mortality. Epidemiol Infect. 2011;139(11):1740–1749. - PubMed
-
- Magiorakos AP, Srinivasan A, Carey RB, et al. . Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous