

Neuroinflammation as a Key Driver of Secondary Neurodegeneration Following Stroke?
- PMID: 34884906
- PMCID: PMC8658328
- DOI: 10.3390/ijms222313101
Neuroinflammation as a Key Driver of Secondary Neurodegeneration Following Stroke?
Abstract
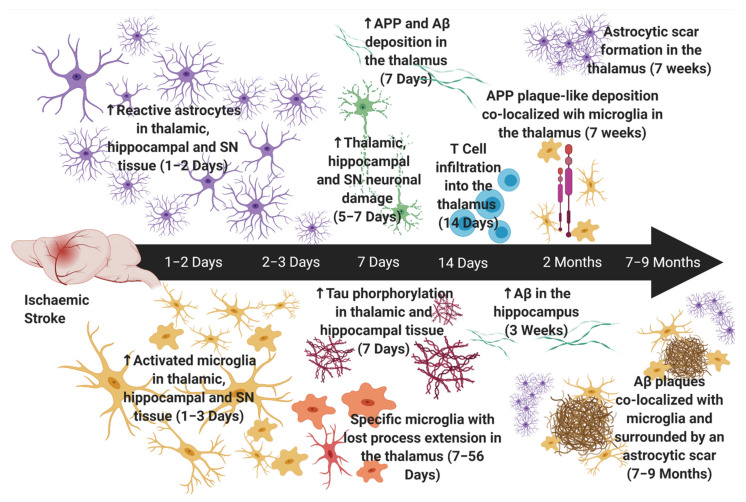
Ischaemic stroke involves the rapid onset of focal neurological dysfunction, most commonly due to an arterial blockage in a specific region of the brain. Stroke is a leading cause of death and common cause of disability, with over 17 million people worldwide suffering from a stroke each year. It is now well-documented that neuroinflammation and immune mediators play a key role in acute and long-term neuronal tissue damage and healing, not only in the infarct core but also in distal regions. Importantly, in these distal regions, termed sites of secondary neurodegeneration (SND), spikes in neuroinflammation may be seen sometime after the initial stroke onset, but prior to the presence of the neuronal tissue damage within these regions. However, it is key to acknowledge that, despite the mounting information describing neuroinflammation following ischaemic stroke, the exact mechanisms whereby inflammatory cells and their mediators drive stroke-induced neuroinflammation are still not fully understood. As a result, current anti-inflammatory treatments have failed to show efficacy in clinical trials. In this review we discuss the complexities of post-stroke neuroinflammation, specifically how it affects neuronal tissue and post-stroke outcome acutely, chronically, and in sites of SND. We then discuss current and previously assessed anti-inflammatory therapies, with a particular focus on how failed anti-inflammatories may be repurposed to target SND-associated neuroinflammation.
Keywords: anti-inflammatories; astrocytes; cerebral ischaemia; dementia; inflammation; microglia; neuroprotection; stroke; therapeutic.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The "Dialogue" Between Central and Peripheral Immunity After Ischemic Stroke: Focus on Spleen.Front Immunol. 2021 Dec 16;12:792522. doi: 10.3389/fimmu.2021.792522. eCollection 2021. Front Immunol. 2021. PMID: 34975893 Free PMC article. Review.
-
Ischemic stroke and diabetes: a TLR4-mediated neuroinflammatory perspective.J Mol Med (Berl). 2024 Jun;102(6):709-717. doi: 10.1007/s00109-024-02441-9. Epub 2024 Mar 28. J Mol Med (Berl). 2024. PMID: 38538987 Review.
-
The Role of Immune Cells in Post-Stroke Angiogenesis and Neuronal Remodeling: The Known and the Unknown.Front Immunol. 2021 Dec 16;12:784098. doi: 10.3389/fimmu.2021.784098. eCollection 2021. Front Immunol. 2021. PMID: 34975872 Free PMC article. Review.
-
Examining the Impact of Microglia on Ischemic Stroke With an Emphasis on the Metabolism of Immune Cells.CNS Neurosci Ther. 2025 Feb;31(2):e70229. doi: 10.1111/cns.70229. CNS Neurosci Ther. 2025. PMID: 39945118 Free PMC article. Review.
-
How cytosolic compartments play safeguard functions against neuroinflammation and cell death in cerebral ischemia.Metab Brain Dis. 2021 Oct;36(7):1445-1467. doi: 10.1007/s11011-021-00770-z. Epub 2021 Jun 26. Metab Brain Dis. 2021. PMID: 34173922 Review.
Cited by
-
From static to dynamic: live observation of the support system after ischemic stroke by two photon-excited fluorescence laser-scanning microscopy.Neural Regen Res. 2023 Oct;18(10):2093-2107. doi: 10.4103/1673-5374.369099. Neural Regen Res. 2023. PMID: 37056116 Free PMC article. Review.
-
Elastin-like polypeptide delivery of anti-inflammatory peptides to the brain following ischemic stroke.bioRxiv [Preprint]. 2023 Mar 15:2023.03.15.532834. doi: 10.1101/2023.03.15.532834. bioRxiv. 2023. Update in: FASEB J. 2023 Aug;37(8):e23077. doi: 10.1096/fj.202300309RR. PMID: 36993686 Free PMC article. Updated. Preprint.
-
The Multifaceted Role of Cofilin in Neurodegeneration and Stroke: Insights into Pathogenesis and Targeting as a Therapy.Cells. 2024 Jan 18;13(2):188. doi: 10.3390/cells13020188. Cells. 2024. PMID: 38247879 Free PMC article. Review.
-
Shared metabolic shifts in endothelial cells in stroke and Alzheimer's disease revealed by integrated analysis.Sci Data. 2023 Sep 29;10(1):666. doi: 10.1038/s41597-023-02512-5. Sci Data. 2023. PMID: 37775708 Free PMC article.
-
Platelets, Thromboinflammation and Neurovascular Disease.Front Immunol. 2022 Mar 4;13:843404. doi: 10.3389/fimmu.2022.843404. eCollection 2022. Front Immunol. 2022. PMID: 35309326 Free PMC article. Review.
References
-
- GBD 2016 Lifetime Risk of Stroke Collaborators. Feigin V.L., Nguyen G., Cercy K., Johnson C.O., Alam T., Parmar P.G., Abajobir A.A., Abate K.H., Abd-Allah F., et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N. Engl. J. Med. 2018;379:2429–2437. doi: 10.1056/NEJMoa1804492. - DOI - PMC - PubMed
-
- World Health Organization The Atlas of Heart Disease and Stroke. [(accessed on 6 March 2021)]. Available online: https://www.who.int/cardiovascular_diseases/resources/atlas/en/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
