

Childhood Malignant Brain Tumors: Balancing the Bench and Bedside
- PMID: 34885207
- PMCID: PMC8656510
- DOI: 10.3390/cancers13236099
Childhood Malignant Brain Tumors: Balancing the Bench and Bedside
Abstract
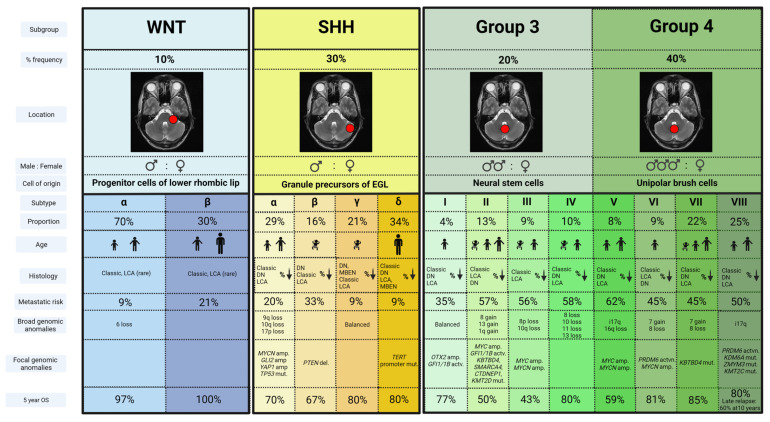
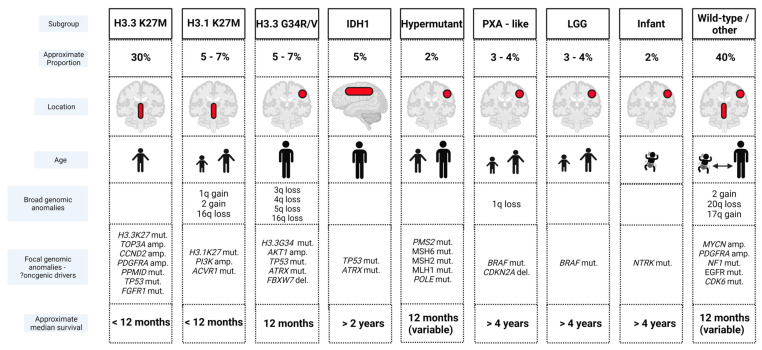
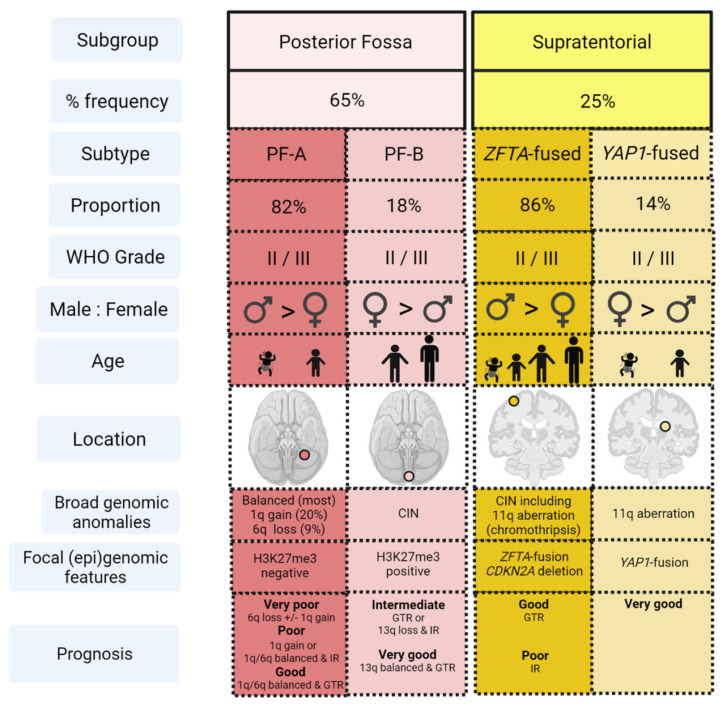
Brain tumors are the leading cause of childhood cancer deaths in developed countries. They also represent the most common solid tumor in this age group, accounting for approximately one-quarter of all pediatric cancers. Developments in neuro-imaging, neurosurgical techniques, adjuvant therapy and supportive care have improved survival rates for certain tumors, allowing a future focus on optimizing cure, whilst minimizing long-term adverse effects. Recent times have witnessed a rapid evolution in the molecular characterization of several of the common pediatric brain tumors, allowing unique clinical and biological patient subgroups to be identified. However, a resulting paradigm shift in both translational therapy and subsequent survival for many of these tumors remains elusive, while recurrence remains a great clinical challenge. This review will provide an insight into the key molecular developments and global co-operative trial results for the most common malignant pediatric brain tumors (medulloblastoma, high-grade gliomas and ependymoma), highlighting potential future directions for management, including novel therapeutic options, and critical challenges that remain unsolved.
Keywords: brain; ependymoma; glioma; medulloblastoma; pediatric; tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Packer R.J., Gajjar A., Vezina G., Rorke-Adams L., Burger P.C., Robertson P.L., Bayer L., LaFond D., Donahue B.R., Marymont M.H., et al. Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J. Clin. Oncol. 2006;24:4202–4208. doi: 10.1200/JCO.2006.06.4980. - DOI - PubMed
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
