

Failure to rescue: A candidate quality metric for durable left ventricular assist device implantation
- PMID: 34887093
- PMCID: PMC9081291
- DOI: 10.1016/j.jtcvs.2021.10.054
Failure to rescue: A candidate quality metric for durable left ventricular assist device implantation
Abstract
Objective: Failure to rescue (FTR), defined as death after a complication, is recognized as a principal driver of variation in mortality among hospitals. We evaluated FTR as a quality metric in patients who received durable left ventricular assist devices (LVADs) using the Society of Thoracic Surgeons Interagency Registry for Mechanically Assisted Circulatory Support.
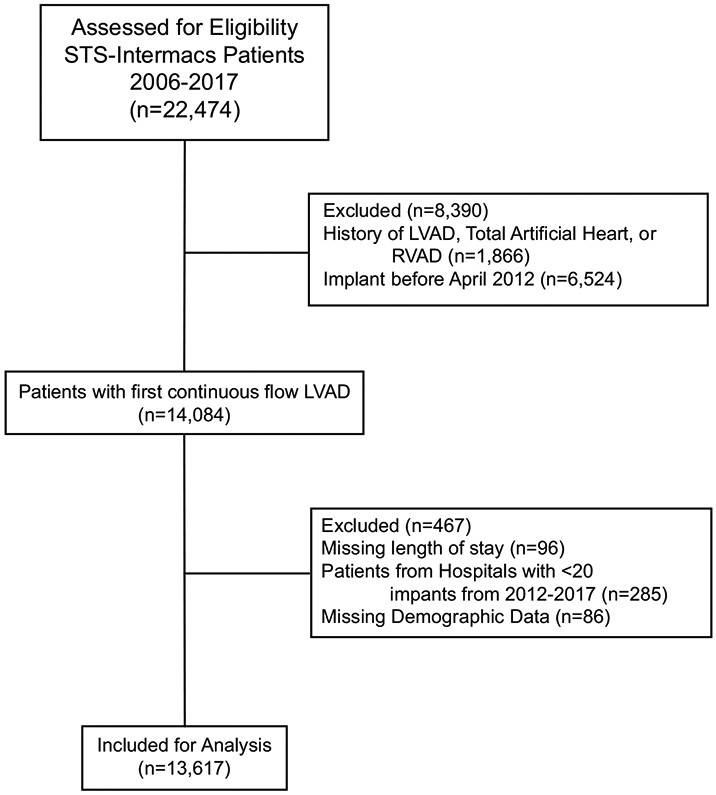
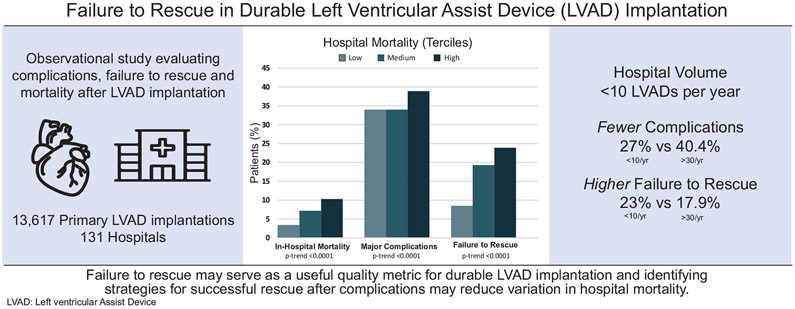
Methods: Data on 13,617 patients who received primary durable LVADs from April 2012 to October 2017 at 131 hospitals that performed at least 20 implants were analyzed from the Society of Thoracic Surgeons Interagency Registry for Mechanically Assisted Circulatory Support. Rates of major complications and FTR were compared across risk-adjusted in-hospital mortality terciles (low, medium, high) and hospital volume. Logistic regression was used to estimate expected FTR rates on the basis of patient factors for each major complication.
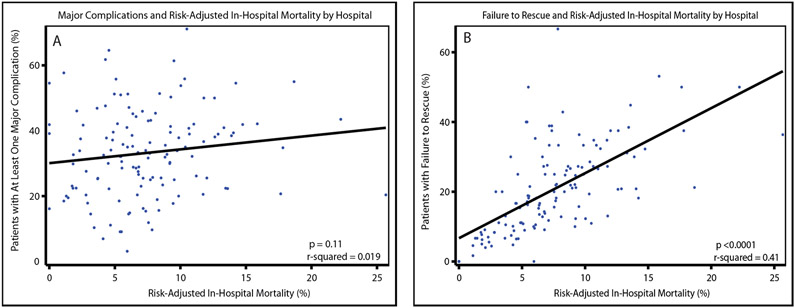
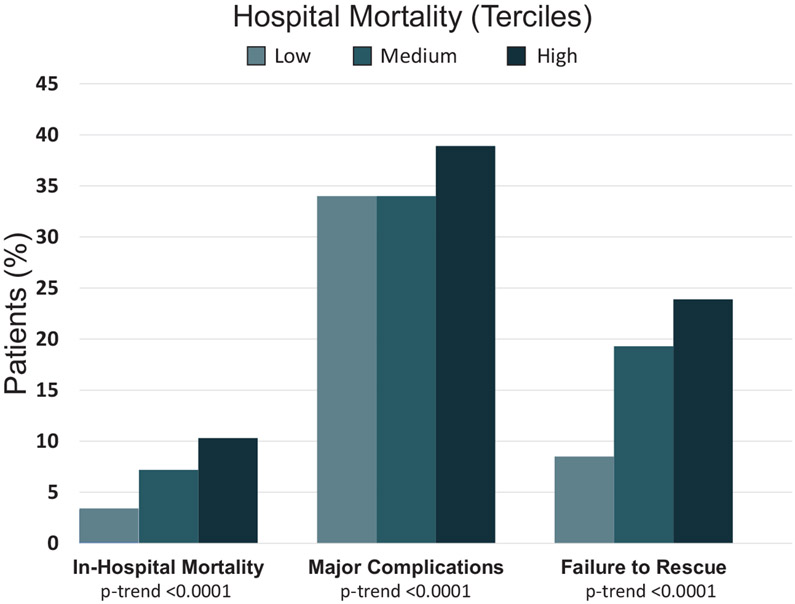
Results: The overall unadjusted in-hospital mortality rate was 6.96%. Risk-adjusted in-hospital mortality rates varied 3.1-fold across terciles (low, 3.3%; high, 10.3%; P trend <.001). Rates of major complications varied 1.1-fold (low, 34.0%; high, 38.8%; P < .0001). Among patients with a major complication, 854 died in-hospital for an FTR rate of 17.7%, with 2.8-fold variation across mortality terciles (low, 8.5%; high, 23.9%; P < .0001). FTR rates were highest for renal dysfunction requiring dialysis (45.3%) and stroke (36.5%). Higher average annual LVAD volume was associated with higher rates of major complications (<10 per year, 26.7%; 10-20 per year, 34.0%; 20-30 per year, 34.0%; >30 per year, 40.1%; P trend <.0001) whereas hospitals implanting <10 per year had the highest FTR rate (<10 per year, 23.5%; 10-20 per year, 16.5%; 20-30 per year, 17.0%; >30 per year, 17.9%; P = .03).
Conclusions: FTR might serve as an important quality metric for durable LVAD implant procedures, and identifying strategies for successful rescue after complications might reduce hospital variations in mortality.
Keywords: LVAD; complications; failure to rescue; left ventricular assist device; mortality.
Copyright © 2021 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Commentary: Left ventricular assist device implantation and failure to rescue: New insights and familiar challenges.J Thorac Cardiovasc Surg. 2023 Jun;165(6):2124-2125. doi: 10.1016/j.jtcvs.2021.11.011. Epub 2021 Nov 12. J Thorac Cardiovasc Surg. 2023. PMID: 34862053 No abstract available.
References
-
- Teuteberg JJ, Cleveland JC Jr, Cowger J, Higgins RS, Goldstein DJ, Keebler M, et al. The Society of Thoracic Surgeons Intermacs 2019 Annual Report: The Changing Landscape of Devices and Indications. Ann Thorac Surg. 2020;109(3):649–660. - PubMed
-
- D’Agostino RS, Jacobs JP, Badhwar V, Paone G, Rankin JS, Han JM, et al. The Society of Thoracic Surgeons Adult Cardiac Surgery Database: 2016 Update on Outcomes and Quality. Ann Thorac Surg. 2016;101(1):24–32. - PubMed
-
- Briasoulis A, Inampudi C, Akintoye E, Adegbala O, Asleh R, Alvarez P, et al. Regional Variation in Mortality, Major Complications, and Cost After Left Ventricular Assist Device Implantation in the United States (2009 to 2014). Am J Cardiol. 2018;121(12):1575–1580. - PubMed
-
- Shah N, Chothani A, Agarwal V, Deshmukh A, Patel N, Garg J, et al. Impact of Annual Hospital Volume on Outcomes after Left Ventricular Assist Device (LVAD) Implantation in the Contemporary Era. J Card Fail. 2016;22(3):232–237. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
