

Efficacy and safety of as-needed albuterol/budesonide versus albuterol in adults and children aged ≥4 years with moderate-to-severe asthma: rationale and design of the randomised, double-blind, active-controlled MANDALA study
- PMID: 34887317
- PMCID: PMC8663093
- DOI: 10.1136/bmjresp-2021-001077
Efficacy and safety of as-needed albuterol/budesonide versus albuterol in adults and children aged ≥4 years with moderate-to-severe asthma: rationale and design of the randomised, double-blind, active-controlled MANDALA study
Abstract
Introduction: Uncontrolled asthma is associated with substantial morbidity. While fast-acting bronchodilators provide quick relief from asthma symptoms, their use as rescue fails to address the underlying inflammation. Combining a short-acting beta2-agonist, such as albuterol (salbutamol), with an inhaled corticosteroid, such as budesonide, in a single inhaler as rescue therapy could help control both bronchoconstriction and inflammation, and reduce the risk of asthma exacerbations.
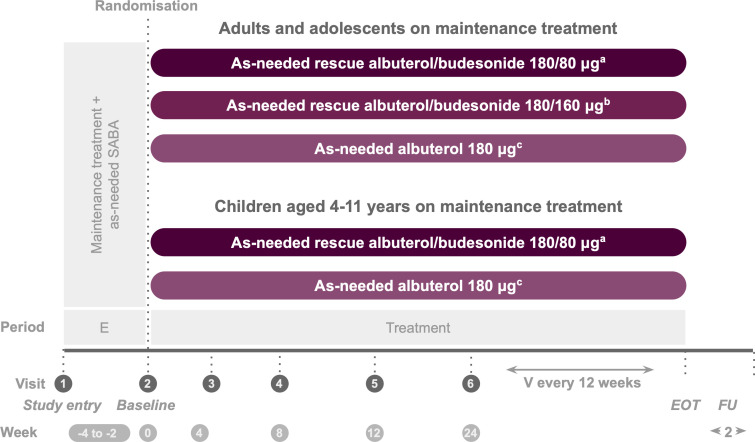
Methods and analysis: The Phase 3 MANDALA study was designed to determine the efficacy of albuterol in combination with budesonide (albuterol/budesonide 180/160 µg or 180/80 µg, two actuations of 90/80 µg or 90/40 µg, respectively) versus albuterol (180 µg, two actuations of 90 µg) as rescue therapy in adult, adolescent and paediatric patients with moderate-to-severe asthma. This event-driven study enrolled symptomatic patients (3000 adults/adolescents and 100 children aged 4-11 years) who experienced ≥1 severe asthma exacerbation in the previous year and were receiving maintenance therapy for ≥3 months prior to study entry. The primary efficacy endpoint was time-to-first severe asthma exacerbation.
Ethics and dissemination: The study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki, and that are consistent with International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use and Good Clinical Practice and the applicable regulatory requirements.
Trial registration: NCT03769090.
Keywords: asthma; asthma in primary care; paediatric asthma.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: BEC is an advisor for, has received consultancy fees from, and is on the speakers’ bureau for AstraZeneca, Boehringer Ingelheim, Genentech, GlaxoSmithKline, Novartis, Regeneron and Sanofi Genzyme. FCA is an employee of Avillion. LR was an employee of Avillion when the study was conducted. EJ and CC are employees of AstraZeneca. AP reports grants, personal fees, non-financial support and other from GlaxoSmithKline, Boehringer Ingelheim, Chiesi Farmaceutici, TEVA, grants, personal fees and non-financial support from AstraZeneca and Menarini, personal fees, non-financial support and other from Mundipharma, Zambon, Novartis and Sanofi/Regeneron, personal fees from Roche and Edmondpharma and grants from Fondazione Maugeri and Fondazione Chiesi, outside the submitted work.
Figures
References
-
- National Institute for Health (NIH), National Heart, Lung, and Blood Institute . Expert panel report 3: guidelines for the diagnosis and management of asthma (EPR-3), 2007. Available: www.nhlbi.nih.gov/guidelines/asthma
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical