

Hormone-Replacement Therapy and Its Association with Breast Cancer Subtypes: A Large Retrospective Cohort Study
- PMID: 34887685
- PMCID: PMC8651048
- DOI: 10.2147/IJWH.S311696
Hormone-Replacement Therapy and Its Association with Breast Cancer Subtypes: A Large Retrospective Cohort Study
Abstract
Purpose: The study examined trends in breast cancer incidence, mammography testing rates, hormone-replacement therapy (HRT) use and breast cancer subtypes in a large Israeli health maintenance organization during 2000-2014.
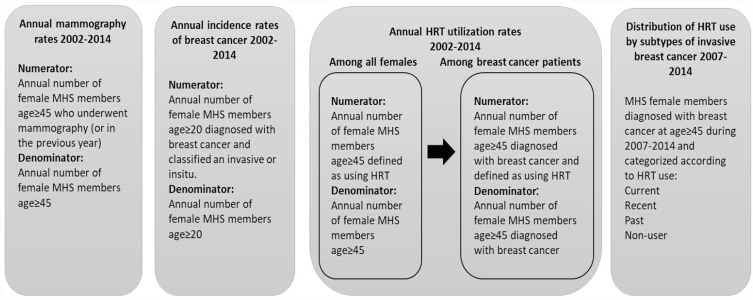
Methods: Annual rates of mammography tests and HRTs use were analyzed in women age ≥45. Annual incidence rates of breast cancer were analyzed in women age ≥20. Estimated annual percentage changes were used to test changes in incidence rates. Invasive breast cancer subtypes were approximated by treatments received. We compared annual rates and duration of HRTs use between women diagnosed with breast cancer and those who were not, as well as HRT use between subtypes of invasive breast cancer.
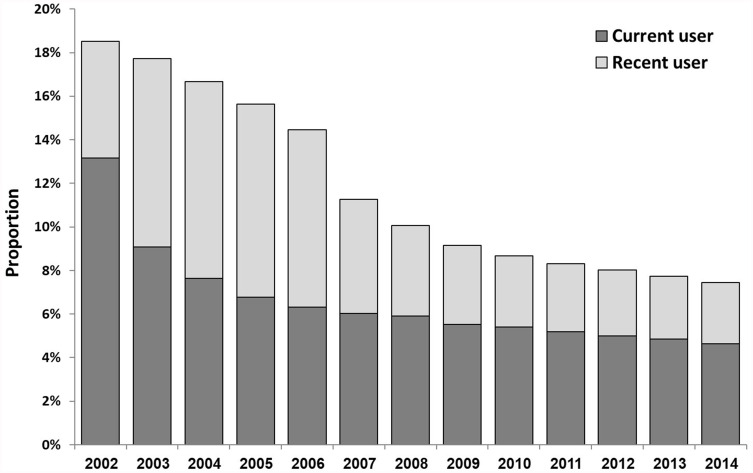
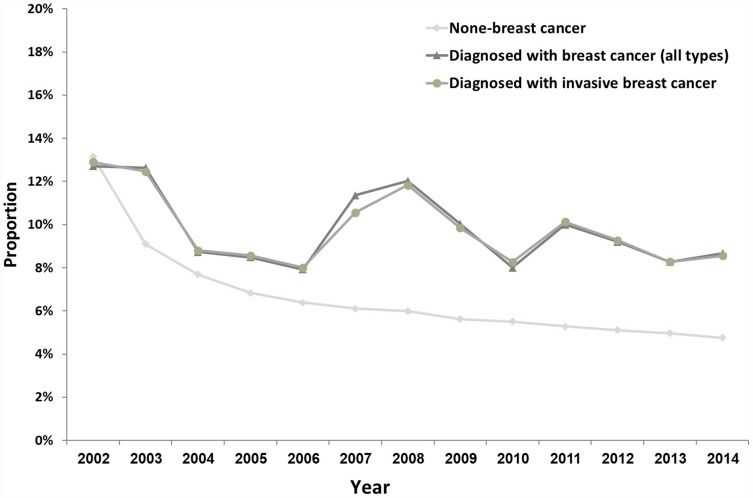
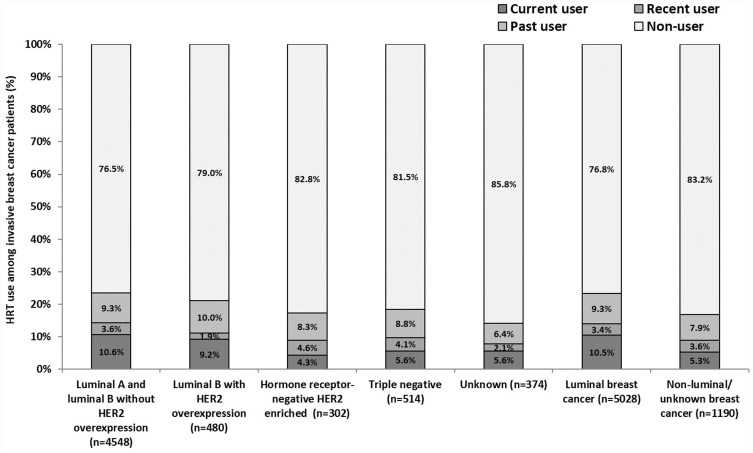
Results: We identified 14,092 breast cancer cases (88% invasive, 12% in situ). The age-adjusted incidence rate of invasive breast cancer peaked in 2005, consistent with increased mammography screening that year, and decreased thereafter. HRT use decreased from 13.2% in 2002 to 4.6% in 2014. The subtypes distribution of 7771 patients diagnosed with invasive breast cancer during 2007-2014 was: luminal A and B without HER2 over-expression (HR+/HER2-), 69.7%; Luminal B with HER2 over-expression (HR+/HER2+), 8.9%; Hormone receptor-negative HER2 enriched (HR-/HER2+), 5.4%; triple negative (HR-/HER2-), 10.0%; unknown, 6.0%. Overall, in women age ≥45 diagnosed with invasive breast cancer, 76-86% did not have HRT exposure vs 14-24% who were current (within 1 year before the breast cancer diagnosis), recent (within 2-5 years), or past users (>5 years). Current/recent HRT use was statistically significantly higher in luminal vs non-luminal/unknown breast cancer subtypes (13.9% vs 8.9%, respectively; p < 0.001).
Conclusion: Our results show a decrease in breast cancer incidence that parallels the global and local decrease in HRT use. Yet, our results imply that current/recent HRT exposure may contribute to the incidence of luminal breast cancer tumors in particular. The magnitude of the effect supports findings from population-based studies.
Keywords: breast cancer; epidemiology; hormone-replacement therapy; incidence; mammography.
© 2021 Rosenberg et al.
Conflict of interest statement
ABS is a medical writer contracted by Pfizer. The remaining authors declare no conflicts of interest.
Figures

Similar articles
-
Parity, hormones and breast cancer subtypes - results from a large nested case-control study in a national screening program.Breast Cancer Res. 2017 Jan 23;19(1):10. doi: 10.1186/s13058-016-0798-x. Breast Cancer Res. 2017. PMID: 28114999 Free PMC article.
-
Risk factors for HR- and HER2-defined breast cancer in Slovenian postmenopausal women.Climacteric. 2012 Feb;15(1):68-74. doi: 10.3109/13697137.2011.609286. Epub 2011 Dec 1. Climacteric. 2012. PMID: 22132797
-
Higher Detection Rates of Biologically Aggressive Breast Cancers in Mammography Screening than in the Biennial Interval.Rofo. 2019 Feb;191(2):130-136. doi: 10.1055/a-0657-3970. Epub 2018 Aug 13. Rofo. 2019. PMID: 30103233 English, German.
-
Molecular breast cancer subtypes and therapies in a public hospital of northeastern Brazil.BMC Womens Health. 2014 Sep 12;14:110. doi: 10.1186/1472-6874-14-110. BMC Womens Health. 2014. PMID: 25216732 Free PMC article.
-
Interactions of hormone replacement therapy, body weight, and bilateral oophorectomy in breast cancer risk.Clin Cancer Res. 2014 Mar 1;20(5):1169-78. doi: 10.1158/1078-0432.CCR-13-2094. Epub 2014 Jan 14. Clin Cancer Res. 2014. PMID: 24423614 Free PMC article.
Cited by
-
Macrophages: Key Players in the Battle against Triple-Negative Breast Cancer.Int J Mol Sci. 2024 Oct 7;25(19):10781. doi: 10.3390/ijms251910781. Int J Mol Sci. 2024. PMID: 39409110 Free PMC article. Review.
-
The association between different hormone replacement therapy use and the incidence of lung cancer: a systematic review and meta-analysis.J Thorac Dis. 2022 Feb;14(2):381-395. doi: 10.21037/jtd-22-48. J Thorac Dis. 2022. PMID: 35280481 Free PMC article.
References
-
- Fitzmaurice C, Abate D, Abbasi N, et al.. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: a systematic analysis for the global burden of disease study. JAMA Oncol. 2019;5:1749–1768. - PMC - PubMed
-
- Health at a glance 2017: OECD indicators. Available from: http://www.oecd.org/health/health-systems/health-at-a-glance-19991312.htm. Accessed November 19, 2021.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
