

Smoldering multiple myeloma: evolving diagnostic criteria and treatment strategies
- PMID: 34889380
- PMCID: PMC8791169
- DOI: 10.1182/hematology.2021000304
Smoldering multiple myeloma: evolving diagnostic criteria and treatment strategies
Abstract
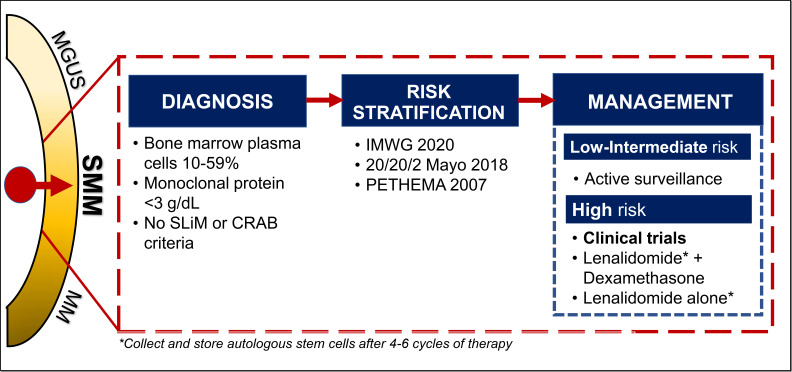
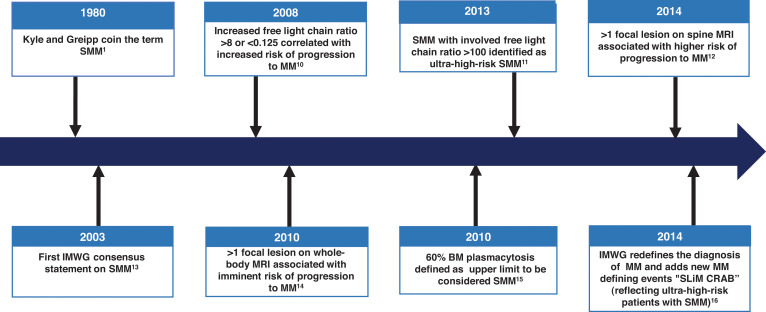
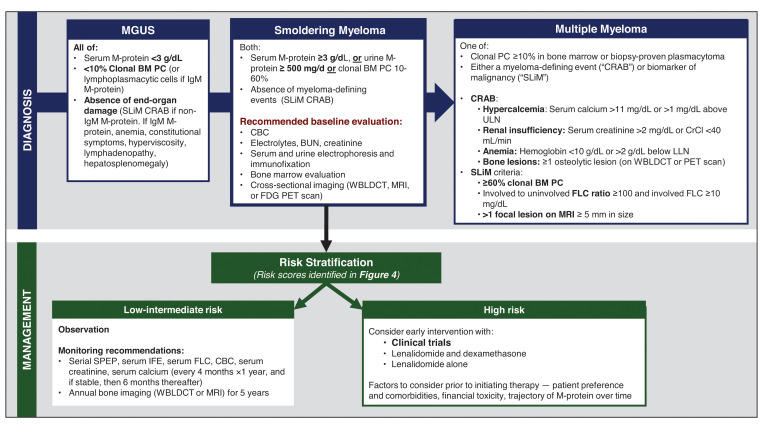
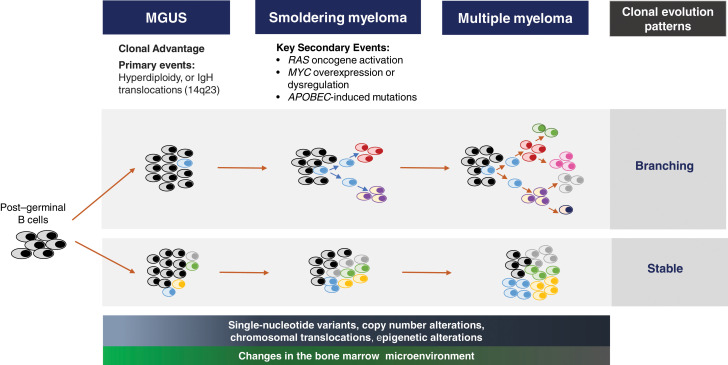
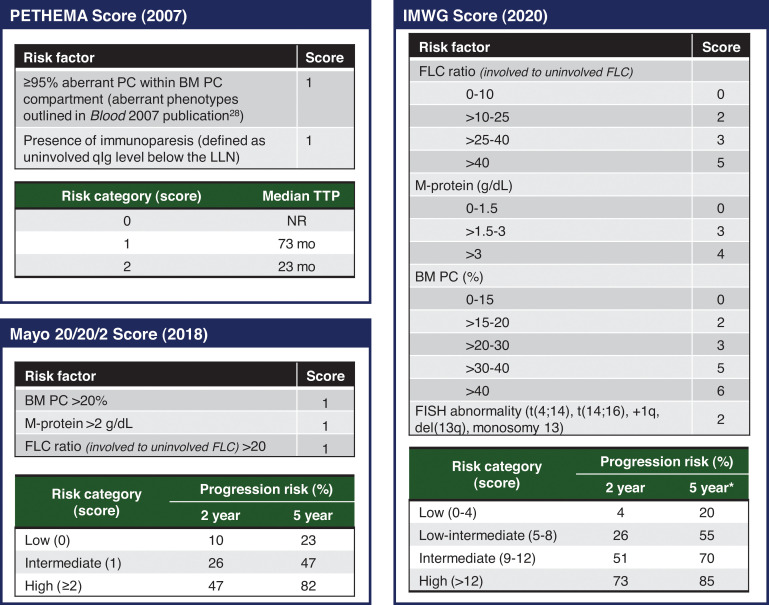
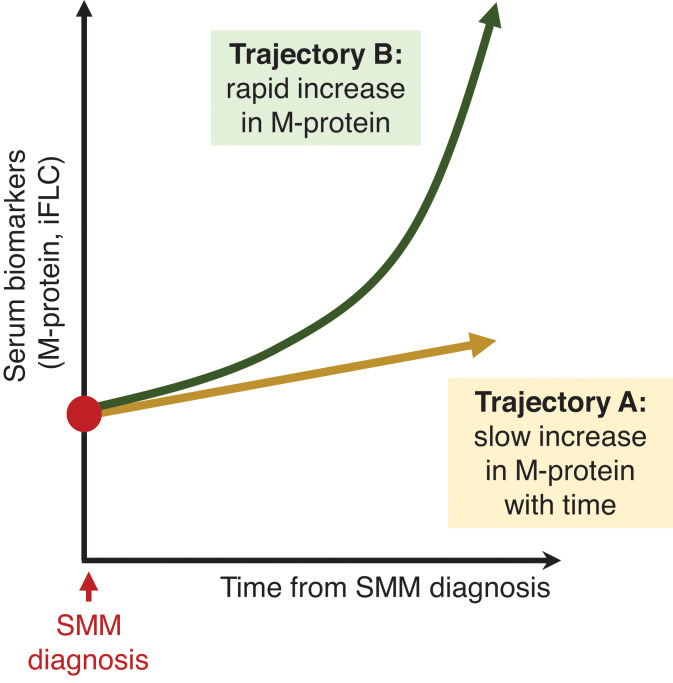
The adage for smoldering myeloma (SMM) has been to observe without treatment, until criteria for active multiple myeloma were satisfied. Definitions and risk stratification models have become more sophisticated, with prognostication tailored to include high-risk cytogenetics as per the most recent International Myeloma Working Group 2020 risk model. Moreover, progress in defining genomic evolution and changes in the bone marrow microenvironment through the monoclonal continuum have given insight into the complexities underlying the different patterns of progression observed in SMM. Given recent data showing improved progression-free survival with early intervention in high-risk SMM, the current dilemma is focused on how these patients should be treated. This case-based article maps the significant advancements made in the diagnosis and risk stratification of SMM. Data from landmark clinical trials will also be discussed, and ongoing trials are summarized. Ultimately, we outline our approach to SMM and hope to impart to the reader a sound concept of the current clinical management of SMM.
Copyright © 2021 by The American Society of Hematology.
Conflict of interest statement
Alissa Visram: no conflicts to disclose.
Joselle Cook: no conflicts to disclose.
Rahma Warsame: no conflicts to disclose.
Figures
References
-
- Chamoun K, Kyasaram RK, Metheny LL, et al.. Demographic characteristics of smoldering multiple myeloma patients: a hospital-based study including 11,643 patients. J Clin Oncol. 2019;37(15, suppl):e13064-e. doi:10.1200/JCO.2019.37.15_suppl.e13064. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources