

Management of hemolytic transfusion reactions
- PMID: 34889404
- PMCID: PMC8791106
- DOI: 10.1182/hematology.2021000308
Management of hemolytic transfusion reactions
Abstract
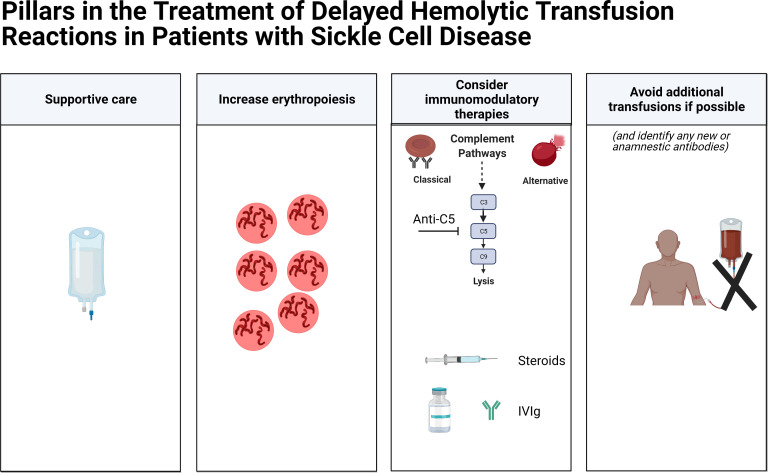
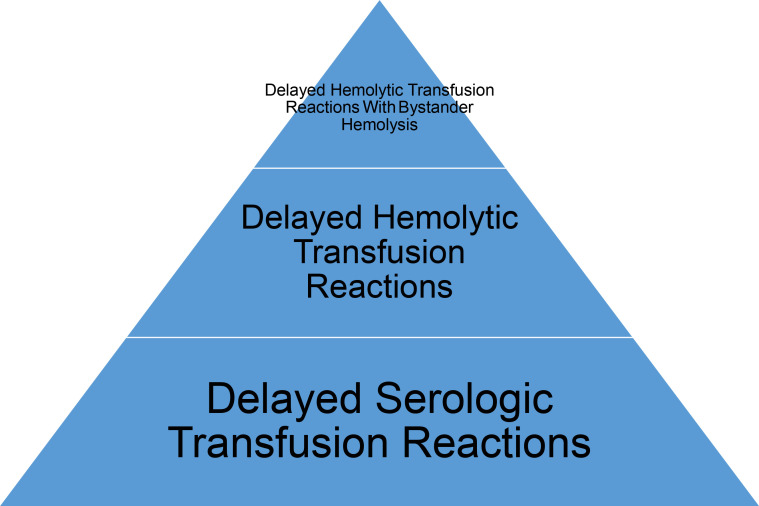
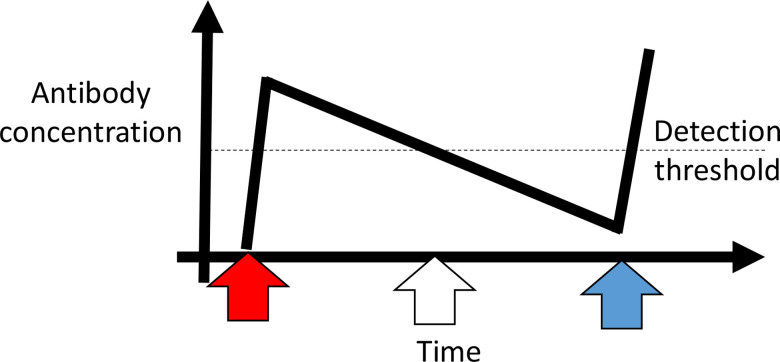
Delayed hemolytic transfusion reactions (DHTRs) in patients with sickle cell disease are underappreciated and potentially fatal. Patients with DHTRs typically have symptoms of pain or dark urine days to weeks following a red blood cell (RBC) transfusion. In instances of DHTRs with hyperhemolysis, the patient's hemoglobin (Hgb) may be significantly lower than it was pretransfusion, and the Hgb A may drop by more than 50%. In most cases, at least 1 RBC alloantibody and sometimes multiple RBC alloantibodies can be identified during the DHTR, with those antibodies presumably having fallen below the level of detection at the time of the implicated transfusion. However, in up to one-third of cases, no new RBC alloantibodies can be identified posttransfusion. Complement is increasingly being appreciated to play a role in DHTRs and hyperhemolysis, not only due to classic pathway activation (with complement fixed antibody bound to RBCs) but also due to alternative pathway activation (resulting in part from plasma free heme). As such, anti-C5 inhibition has recently been reported to be effective at mitigating hemolysis in the setting of some severe DHTRs. Transfusion avoidance during DHTRs is recommended if possible, with long-term transfusion support advice being less clear; for example, a history of a severe DHTR may lead to questions regarding the safety of transfusions prior to curative therapies such as stem cell transplantation or gene therapy. A better understanding of antibody-positive and antibody-negative DHTRs, including patient- or disease-specific risk factors, is necessary to improve transfusion safety.
Copyright © 2021 by The American Society of Hematology.
Conflict of interest statement
Jeanne E. Hendrickson: no competing financial interests to declare.
Ross M. Fasano: no competing financial interests to declare.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). NHSN Biovigilance Component: Hemovigilance Module Surveillance Protocol v2.6. Vol. 2021. CDC; 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous