

Minimal residual disease in multiple myeloma: why, when, where
- PMID: 34889430
- PMCID: PMC8791109
- DOI: 10.1182/hematology.2021000230
Minimal residual disease in multiple myeloma: why, when, where
Abstract
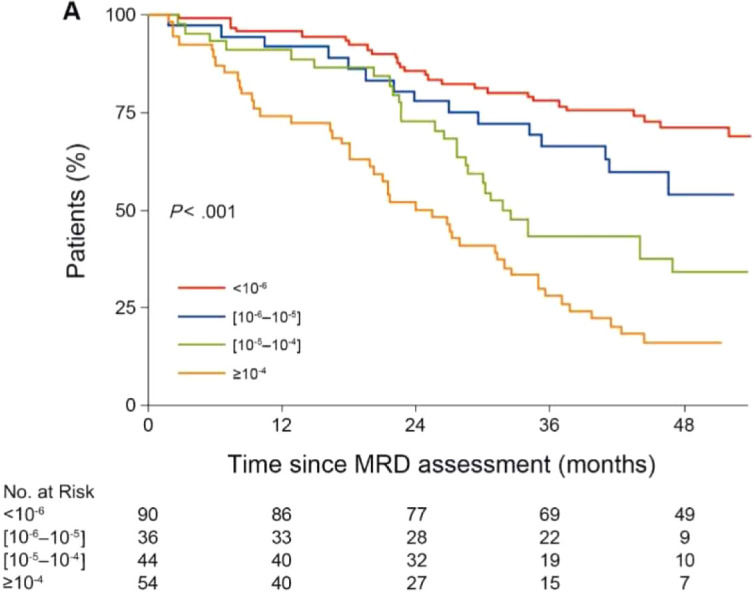
Improvements in multiple myeloma therapy have led to deeper responses that are beyond the limit of detection by historical immunohistochemistry and conventional flow cytometry in bone marrow samples. In parallel, more sensitive techniques for assessing minimal residual disease (MRD) through next-generation flow cytometry and sequencing have been developed and are now routinely available. Deep responses when measured by these assays correspond with improved outcomes and survival. We review the data supporting MRD testing as well as its limitations and how it may fit in with current and future clinical practice.
Copyright © 2021 by The American Society of Hematology.
Conflict of interest statement
Andrew J. Yee has consulted for Adaptive, Amgen, BMS, GSK, Janssen, Karyopharm, Oncopeptides, Sanofi, and Takeda and has received clinical trial support from Adaptive, Amgen, BMS, Janssen, and Takeda.
Noopur Raje has consulted for Amgen, BMS, Bluebird, GSK, Janssen, and Karyopharm; served on scientific advisory board for Caribou and Immuneel; and received research funding from Bluebird.
Figures
Similar articles
-
Prognostic value of sequencing-based minimal residual disease detection in patients with multiple myeloma who underwent autologous stem-cell transplantation.Ann Oncol. 2017 Oct 1;28(10):2503-2510. doi: 10.1093/annonc/mdx340. Ann Oncol. 2017. PMID: 28945825 Free PMC article.
-
Measurable Residual Disease and Decision-Making in Multiple Myeloma.Hematol Oncol Clin North Am. 2024 Apr;38(2):477-495. doi: 10.1016/j.hoc.2023.12.009. Epub 2024 Jan 6. Hematol Oncol Clin North Am. 2024. PMID: 38184470 Review.
-
MRD Assessment in Multiple Myeloma: Progress and Challenges.Curr Hematol Malig Rep. 2021 Apr;16(2):162-171. doi: 10.1007/s11899-021-00633-5. Epub 2021 May 5. Curr Hematol Malig Rep. 2021. PMID: 33950462 Review.
-
Better therapy requires better response evaluation: Paving the way for minimal residual disease testing for every myeloma patient.Cytometry B Clin Cytom. 2016 Jan;90(1):14-20. doi: 10.1002/cyto.b.21273. Epub 2015 Dec 22. Cytometry B Clin Cytom. 2016. PMID: 26147584 Review.
-
Standardizing Clinical Workflow for Assessing Minimal Residual Disease by Flow Cytometry in Multiple Myeloma.Clin Lymphoma Myeloma Leuk. 2023 Jan;23(1):e41-e50. doi: 10.1016/j.clml.2022.10.008. Epub 2022 Oct 22. Clin Lymphoma Myeloma Leuk. 2023. PMID: 36443182 Free PMC article.
Cited by
-
Dynamics of minimal residual disease and its clinical implications in multiple myeloma: A retrospective real-life analysis.Clin Med (Lond). 2024 Nov;24(6):100252. doi: 10.1016/j.clinme.2024.100252. Epub 2024 Oct 1. Clin Med (Lond). 2024. PMID: 39362336 Free PMC article.
-
Recent advances in the management of older adults with newly diagnosed multiple myeloma in Japan.Jpn J Clin Oncol. 2022 Sep 18;52(9):966-974. doi: 10.1093/jjco/hyac111. Jpn J Clin Oncol. 2022. PMID: 35830865 Free PMC article. Review.
-
Monitoring multiple myeloma in the peripheral blood based on cell-free DNA and circulating plasma cells.Ann Hematol. 2022 Apr;101(4):811-824. doi: 10.1007/s00277-022-04771-5. Epub 2022 Feb 1. Ann Hematol. 2022. PMID: 35106639 Free PMC article.
-
Cytogenetic risk stratification combined with minimal residual disease status influences the therapeutic outcome and prognosis of multiple myelomas.Sci Rep. 2025 Apr 12;15(1):12545. doi: 10.1038/s41598-025-97125-w. Sci Rep. 2025. PMID: 40217083 Free PMC article.
-
Multiple Myeloma Insights from Single-Cell Analysis: Clonal Evolution, the Microenvironment, Therapy Evasion, and Clinical Implications.Cancers (Basel). 2025 Feb 14;17(4):653. doi: 10.3390/cancers17040653. Cancers (Basel). 2025. PMID: 40002248 Free PMC article. Review.
References
-
- Cavo M, Zamagni E, Tosi P, et al; Bologna 2002 study. Superiority of thalidomide and dexamethasone over vincristine-doxorubicindexamethasone (VAD) as primary therapy in preparation for autologous transplantation for multiple myeloma. Blood. 2005;106(1):35-39. doi:10.1182/blood-2005-02-0522. - DOI - PubMed
-
- Landgren O, Hultcrantz M, Diamond B, et al.. Safety and effectiveness of weekly carfilzomib, lenalidomide, dexamethasone, and daratumumab combination therapy for patients with newly diagnosed multiple myeloma: the MANHATTAN nonrandomized clinical trial. JAMA Oncol. 2021;7(6):862-868. doi:10.1001/jamaoncol.2021.0611. - DOI - PMC - PubMed
-
- Martinez-Lopez J, Blade J, Mateos M-V, et al; Grupo Español de MM; Programa para el Estudio de la Terapé utica en Hemopatía Maligna. Long-term prognostic significance of response in multiple myeloma after stem cell transplantation. Blood. 2011;118(3):529-534. doi:10.1182/blood-2011-01-332320. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical