

Cognitive Recovery by Decade in Healthy 40- to 80-Year-Old Volunteers After Anesthesia Without Surgery
- PMID: 34889804
- PMCID: PMC8760160
- DOI: 10.1213/ANE.0000000000005824
Cognitive Recovery by Decade in Healthy 40- to 80-Year-Old Volunteers After Anesthesia Without Surgery
Abstract
Background: Postoperative delirium and postoperative cognitive dysfunction are the most common complications for older surgical patients. General anesthesia may contribute to the development of these conditions, but there are little data on the association of age with cognitive recovery from anesthesia in the absence of surgery or underlying medical condition.
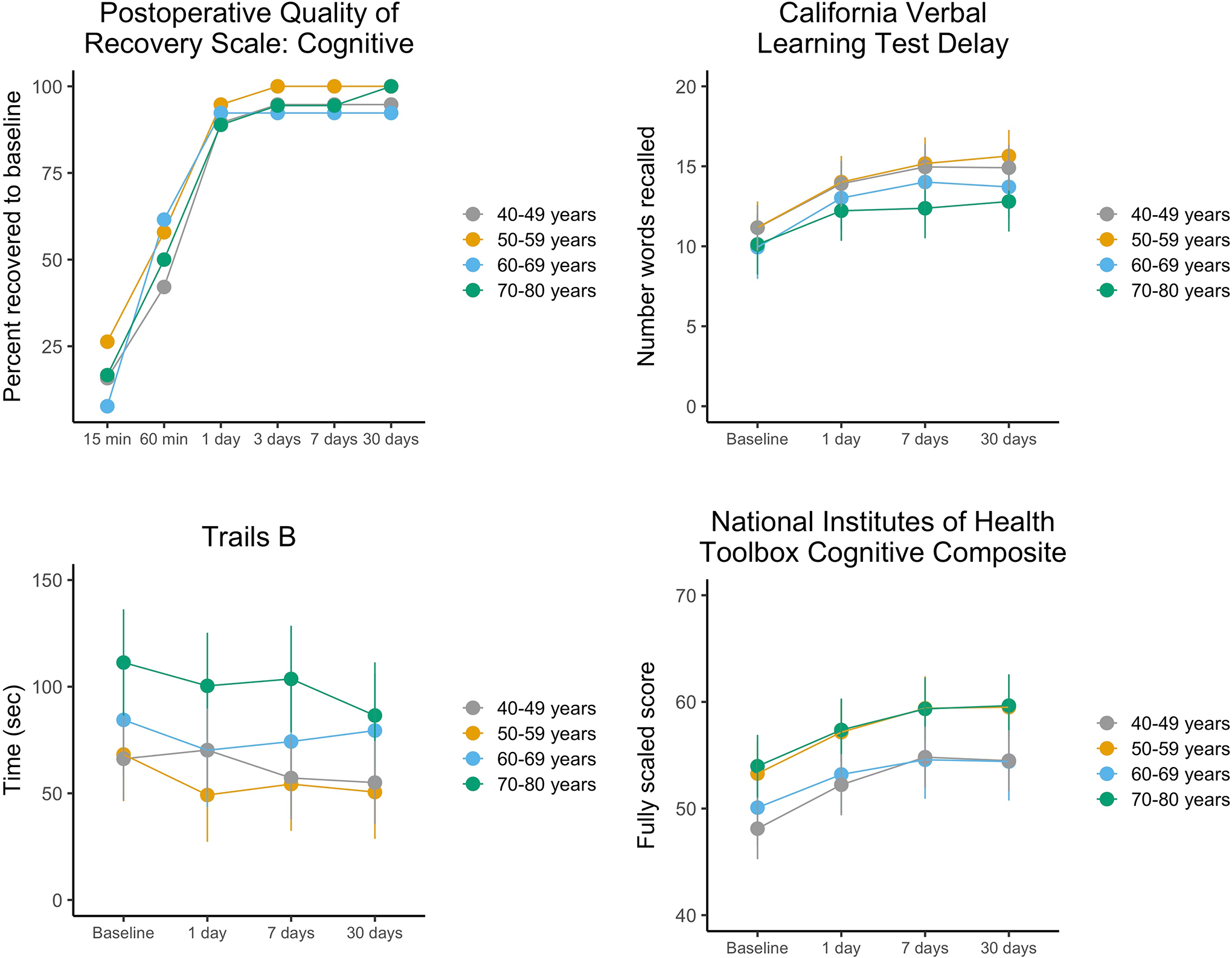
Methods: We performed a single-center cohort study of healthy adult volunteers 40 to 80 years old (N = 71, mean age 58.5 years, and 44% women) with no underlying cognitive dysfunction. Volunteers underwent cognitive testing before and at multiple time points after 2 hours of general anesthesia consisting of propofol induction and sevoflurane maintenance, akin to a general anesthetic for a surgical procedure, although no procedure was performed. The primary outcome was time to recovery to cognitive baseline on the Postoperative Quality of Recovery Scale (PQRS) within 30 days of anesthesia. Secondary cognitive outcomes were time to recovery on in-depth neuropsychological batteries, including the National Institutes of Health Toolbox and well-validated paper-and-pencil tests. The primary hypothesis is that time to recovery of cognitive function after general anesthesia increases across decades from 40 to 80 years of age. We examined this with discrete-time logit regression (for the primary outcome) and linear mixed models for interactions of age decade with time postanesthesia (for secondary outcomes).
Results: There was no association between age group and recovery to baseline on the PQRS; 36 of 69 (52%) recovered within 60-minute postanesthesia and 63 of 69 (91%) by day 1. Hazard ratios (95% confidence interval) for each decade compared to 40- to 49-year olds were: 50 to 59 years, 1.41 (0.50-4.03); 60 to 69 years, 1.03 (0.35-3.00); and 70 to 80 years, 0.69 (0.25-1.88). There were no significant differences between older decades relative to the 40- to 49-year reference decade in recovery to baseline on secondary cognitive measures.
Conclusions: Recovery of cognitive function to baseline was rapid and did not differ between age decades of participants, although the number in each decade was small. These results suggest that anesthesia alone may not be associated with cognitive recovery in healthy adults of any age decade.
Trial registration: ClinicalTrials.gov NCT02275026.
Copyright © 2021 International Anesthesia Research Society.
Conflict of interest statement
Conflicts of interest: See Disclosures at the end of the article.
Figures

References
-
- Evered LA, Silbert BS. Postoperative Cognitive Dysfunction and Noncardiac Surgery. Anesthesia & Analgesia 2018;127:496–505. - PubMed
-
- Witlox J, Eurelings LSM, de Jonghe JFM, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in Elderly Patients and the Risk of Postdischarge Mortality, Institutionalization, and Dementia: A Meta-analysis. JAMA 2010;304:443–51. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
