

COVID-19 symptoms at time of testing and association with positivity among outpatients tested for SARS-CoV-2
- PMID: 34890441
- PMCID: PMC8664207
- DOI: 10.1371/journal.pone.0260879
COVID-19 symptoms at time of testing and association with positivity among outpatients tested for SARS-CoV-2
Abstract
Introduction: Symptoms associated with SARS-CoV-2 infection remain incompletely understood, especially among ambulatory, non-hospitalized individuals. With host factors, symptoms predictive of SARS-CoV-2 could be used to guide testing and intervention strategies.
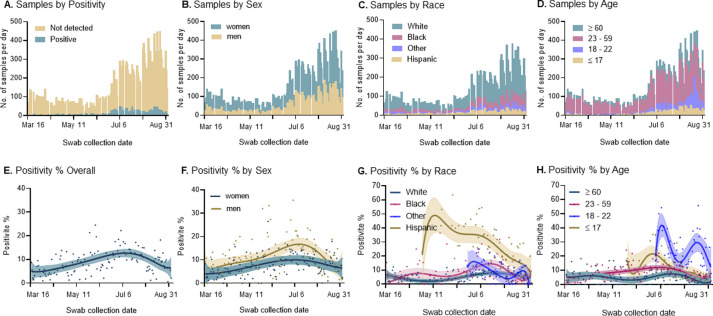
Methods: Between March 16 and September 3, 2020, we examined the characteristics and symptoms reported by individuals presenting to a large outpatient testing program in the Southeastern US for nasopharyngeal SARS-CoV-2 RNA RT-PCR testing. Using self-reported symptoms, demographic characteristics, and exposure and travel histories, we identified the variables associated with testing positive using modified Poisson regression.
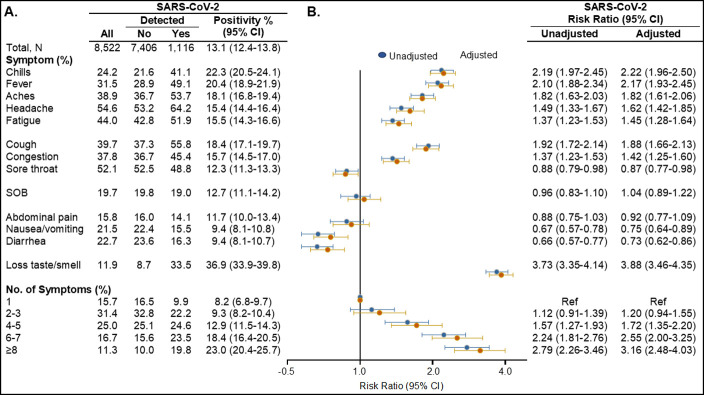
Results: Among 20,177 tested individuals, the proportion positive was 9.4% (95% CI, 9.0-9.8) and was higher for men, younger individuals, and racial/ethnic minorities (all P<0.05); the positivity proportion was higher for Hispanics (26.9%; 95% CI. 24.9-29.0) compared to Blacks (8.6%; 95% CI, 7.6-9.7) or Whites (5.8%; 95% CI, 5.4-6.3). Individuals reporting contact with a COVID-19 case had the highest positivity proportion (22.8%; 95% CI, 21.5-24.1). Among the subset of 8,522 symptomatic adults who presented for testing after May 1, when complete symptom assessments were performed, SARS-CoV-2 RNA PCR was detected in 1,116 (13.1%). Of the reported symptoms, loss of taste or smell was most strongly associated with SARS-CoV-2 RNA detection with an adjusted risk ratio of 3.88 (95% CI, 3.46-4.35). The presence of chills, fever, cough, aches, headache, fatigue and nasal congestion also significantly increased the risk of detecting SARS-CoV-2 RNA, while diarrhea or nausea/vomiting, although not uncommon, were significantly more common in those with a negative test result. Symptom combinations were frequent with 67.9% experiencing ≥4 symptoms, including 19.8% with ≥8 symptoms; report of greater than three symptoms increased the risk of SARS-CoV-2 RNA detection.
Conclusions: In a large outpatient population in the Southeastern US, several symptoms, most notably loss of taste or smell, and greater symptom burden were associated with detection of SARS-CoV-2 RNA. Persons of color and those with who were a contact of a COVID-19 case were also more likely to test positive. These findings suggest that, given limited SARS-CoV-2 testing capacity, symptom presentation and host characteristics can be used to guide testing and intervention prioritization.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Covid-19 presentation among symptomatic healthcare workers in Ireland.Occup Med (Lond). 2021 Apr 9;71(2):95-98. doi: 10.1093/occmed/kqab012. Occup Med (Lond). 2021. PMID: 33585881 Free PMC article.
-
Comparative Analysis of the Clinical Presentation of Individuals Who Test Positive or Negative for SARS-CoV-2: Results from a Test Street Study.Viruses. 2024 Jun 26;16(7):1031. doi: 10.3390/v16071031. Viruses. 2024. PMID: 39066194 Free PMC article.
-
Self-collection and pooling of samples as resources-saving strategies for RT-PCR-based SARS-CoV-2 surveillance, the example of travelers in French Polynesia.PLoS One. 2021 Sep 2;16(9):e0256877. doi: 10.1371/journal.pone.0256877. eCollection 2021. PLoS One. 2021. PMID: 34473769 Free PMC article.
-
Molecular diagnostic approaches for SARS-CoV-2 detection and pathophysiological consequences.Mol Biol Rep. 2023 Dec;50(12):10367-10382. doi: 10.1007/s11033-023-08844-0. Epub 2023 Oct 10. Mol Biol Rep. 2023. PMID: 37817022 Review.
-
JMM Profile: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).J Med Microbiol. 2021 Mar;70(3):001336. doi: 10.1099/jmm.0.001336. Epub 2021 Mar 23. J Med Microbiol. 2021. PMID: 33759741 Free PMC article. Review.
Cited by
-
Novel large empirical study of deep transfer learning for COVID-19 classification based on CT and X-ray images.Sci Rep. 2024 Nov 3;14(1):26520. doi: 10.1038/s41598-024-76498-4. Sci Rep. 2024. PMID: 39489731 Free PMC article.
-
How predictive of SARS-CoV-2 infection are clinical characteristics at presentation among individuals with COVID-like symptoms treated at the Mexican Institute of Social Security.PLoS One. 2023 Dec 21;18(12):e0296320. doi: 10.1371/journal.pone.0296320. eCollection 2023. PLoS One. 2023. PMID: 38128048 Free PMC article.
-
Investigation of the use of a sensor bracelet for the presymptomatic detection of changes in physiological parameters related to COVID-19: an interim analysis of a prospective cohort study (COVI-GAPP).BMJ Open. 2022 Jun 21;12(6):e058274. doi: 10.1136/bmjopen-2021-058274. BMJ Open. 2022. PMID: 35728900 Free PMC article. Clinical Trial.
-
Diagnosis of COVID-19: Is Fever the Best Indicator of COVID-19 in Vaccinated SARS-CoV-2-Positive Adults?Cureus. 2024 Sep 5;16(9):e68749. doi: 10.7759/cureus.68749. eCollection 2024 Sep. Cureus. 2024. PMID: 39371770 Free PMC article.
-
Impaired metal perception and regulation of associated human foliate papillae tongue transcriptome in long-COVID-19.Sci Rep. 2024 Jul 4;14(1):15408. doi: 10.1038/s41598-024-66079-w. Sci Rep. 2024. PMID: 38965271 Free PMC article.
References
-
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. World Health Organization. https://covid19.who.int/. Accessed September 7, 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
