

Junior doctors' experiences with interprofessional collaboration: Wandering the landscape
- PMID: 34890487
- PMCID: PMC9305225
- DOI: 10.1111/medu.14711
Junior doctors' experiences with interprofessional collaboration: Wandering the landscape
Abstract
Context: The transition from medical student to junior doctor is challenging. Junior doctors need to become part of the physician community of practice (CoP), while dealing with new responsibilities, tasks and expectations. At the same time, they need to learn how to navigate the frontiers and intersections with the other communities of practice that form the Landscape of Practice (LoP). This study aims to understand how junior doctors experience interprofessional collaboration (IPC) and what elements shape these experiences considering their transition to clinical practice.
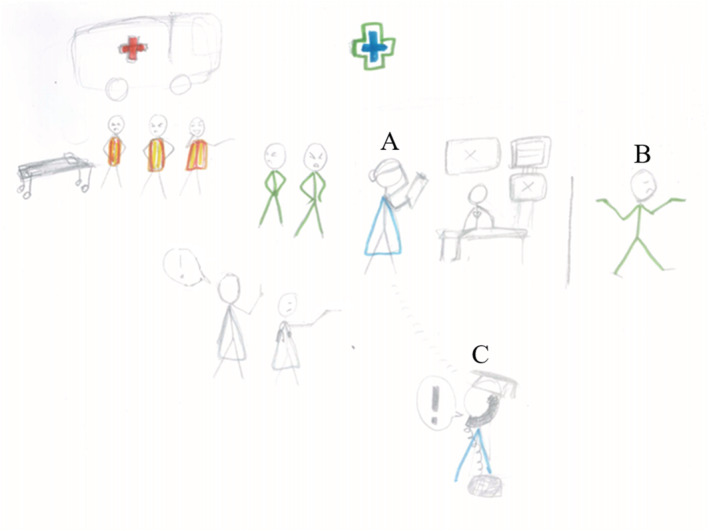
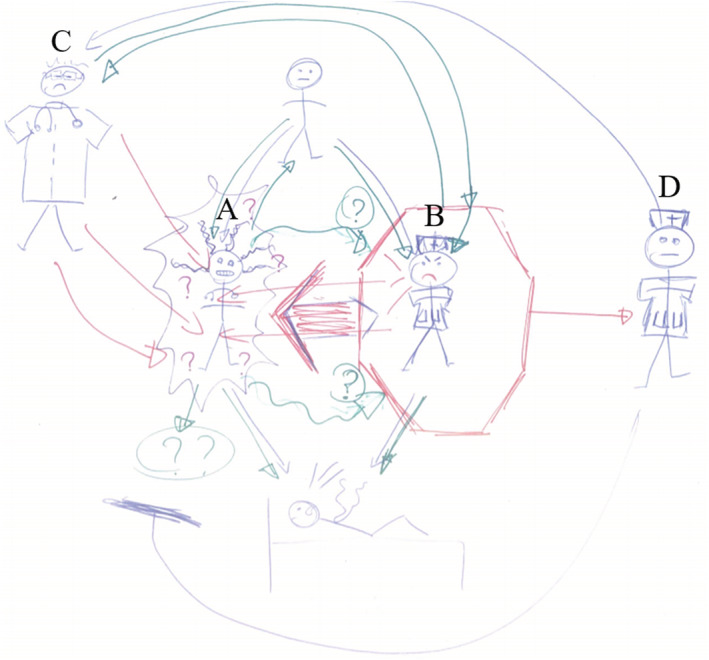
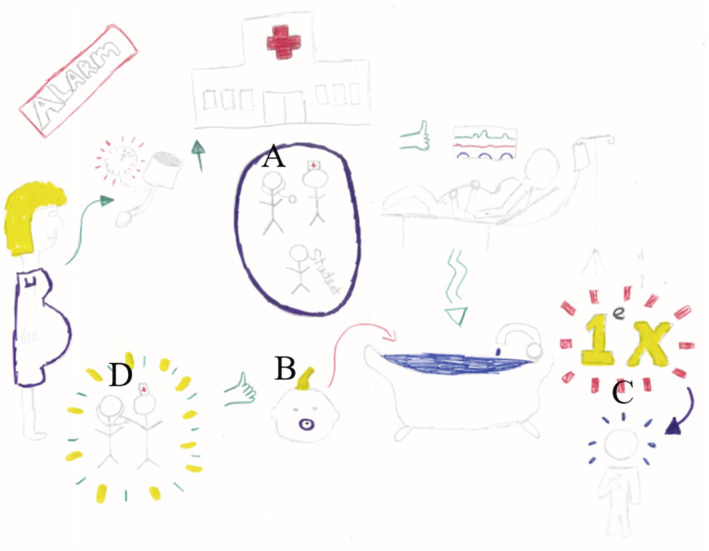
Methods: In this multicentre qualitative study, 13 junior doctors individually drew two rich pictures of IPC experiences, one positive and one negative. A rich picture is a visual representation, a drawing of a particular situation intended to capture the complex and non-verbal elements of an experience. We used semi-structured interviews to deepen the understanding of junior doctors' depicted IPC experiences. We analysed both visual materials and interview transcripts iteratively, for which we adopted an inductive constructivist thematic analysis.
Results: While transitioning into a doctor, junior doctors become foremost members of the physician CoP and shape their professional identity based on perceived values in their physician community. Interprofessional learning occurs implicitly, without input from the interprofessional team. As a result, junior doctors struggle to bridge the gap between themselves and the interprofessional team, preventing IPC learning from developing into an integrative process. This professional isolation leaves junior doctors wandering the landscape of practice without understanding roles, attitudes and expectations of others.
Conclusions: Learning IPC needs to become a collective endeavour and an explicit learning goal, based on multisource feedback to take advantage of the expertise already present in the LoP. Furthermore, junior doctors need a safe environment to embrace and reflect on the emotions aroused by interprofessional interactions, under the guidance of experienced facilitators.
© 2022 The Authors. Medical Education published by Association for the Study of Medical Education and John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Comment in
-
Interprofessional education important for transition to interprofessional collaboration.Med Educ. 2022 May;56(5):585. doi: 10.1111/medu.14730. Epub 2022 Jan 23. Med Educ. 2022. PMID: 35018666 No abstract available.
-
From islander to team player: How to make professional silos more fluid.Med Educ. 2022 May;56(5):586. doi: 10.1111/medu.14747. Epub 2022 Feb 17. Med Educ. 2022. PMID: 35156220 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
