

New method to measure interbreath intervals in infants for the assessment of apnoea and respiration
- PMID: 34893521
- PMCID: PMC8666899
- DOI: 10.1136/bmjresp-2021-001042
New method to measure interbreath intervals in infants for the assessment of apnoea and respiration
Abstract
Background: Respiratory disorders, including apnoea, are common in preterm infants due to their immature respiratory control compared with term-born infants. However, our inability to accurately measure respiratory rate in hospitalised infants results in unreported episodes of apnoea and an incomplete picture of respiratory activity.
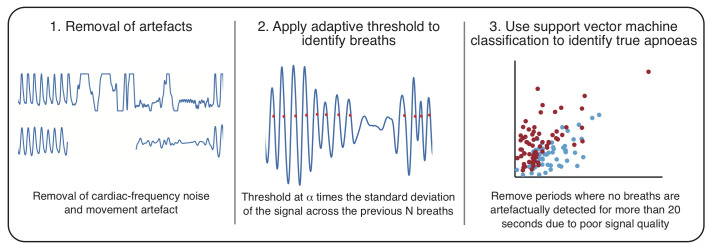
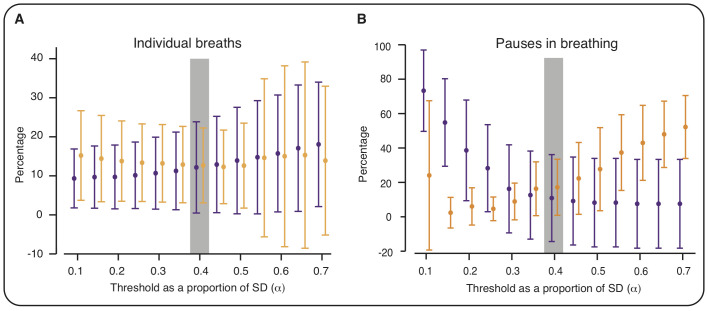
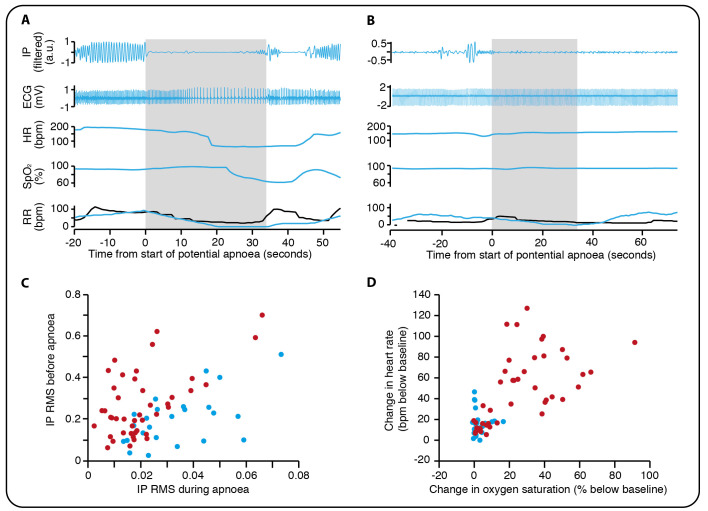
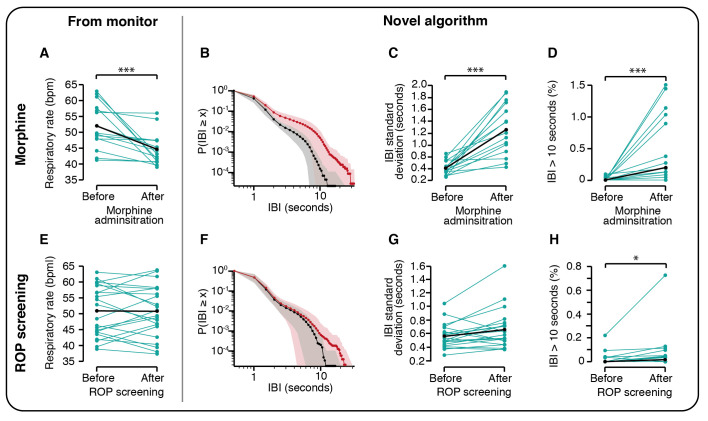
Methods: We develop, validate and use a novel algorithm to identify interbreath intervals (IBIs) and apnoeas in preterm infants. In 42 preterm infants (1600 hours of recordings), we assess IBIs from the chest electrical impedance pneumograph using an adaptive amplitude threshold for the detection of breaths. The algorithm is refined by comparing its accuracy with clinically observed breaths and pauses in breathing. We develop an automated classifier to differentiate periods of true apnoea from artefactually low amplitude signal. We assess the performance of this algorithm in the detection of morphine-induced respiratory depression. Finally, we use the algorithm to investigate whether retinopathy of prematurity (ROP) screening alters the IBI distribution.
Results: Individual breaths were detected with a false-positive rate of 13% and a false-negative rate of 12%. The classifier identified true apnoeas with an accuracy of 93%. As expected, morphine caused a significant shift in the IBI distribution towards longer IBIs. Following ROP screening, there was a significant increase in pauses in breathing that lasted more than 10 s (t-statistic=1.82, p=0.023). This was not reflected by changes in the monitor-derived respiratory rate and no episodes of apnoea were recorded in the medical records.
Conclusions: We show that our algorithm offers an improved method for the identification of IBIs and apnoeas in preterm infants. Following ROP screening, increased respiratory instability can occur even in the absence of clinically significant apnoeas. Accurate assessment of infant respiratory activity is essential to inform clinical practice.
Keywords: respiratory measurement.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials