

Adherence to Antiseizure vs Other Medications Among US Medicare Beneficiaries With and Without Epilepsy
- PMID: 34893556
- PMCID: PMC8793102
- DOI: 10.1212/WNL.0000000000013119
Adherence to Antiseizure vs Other Medications Among US Medicare Beneficiaries With and Without Epilepsy
Abstract
Background and objective: The objectives of this study were to compare adherence to antiseizure medications (ASMs) vs non-ASMs among individuals with epilepsy, to assess the degree to which variation in adherence is due to differences between individuals vs between medication classes among individuals with epilepsy, and to compare adherence in individuals with vs without epilepsy.
Methods: This was a retrospective cohort study using Medicare. We included beneficiaries with epilepsy (≥1 ASM, plus ICD-9-CM diagnostic codes) and a 20% random sample without epilepsy. Adherence for each medication class was measured by the proportion of days covered (PDC) in 2013 to 2015. We used Spearman correlation coefficients, Cohen κ statistics, and multilevel logistic regressions.
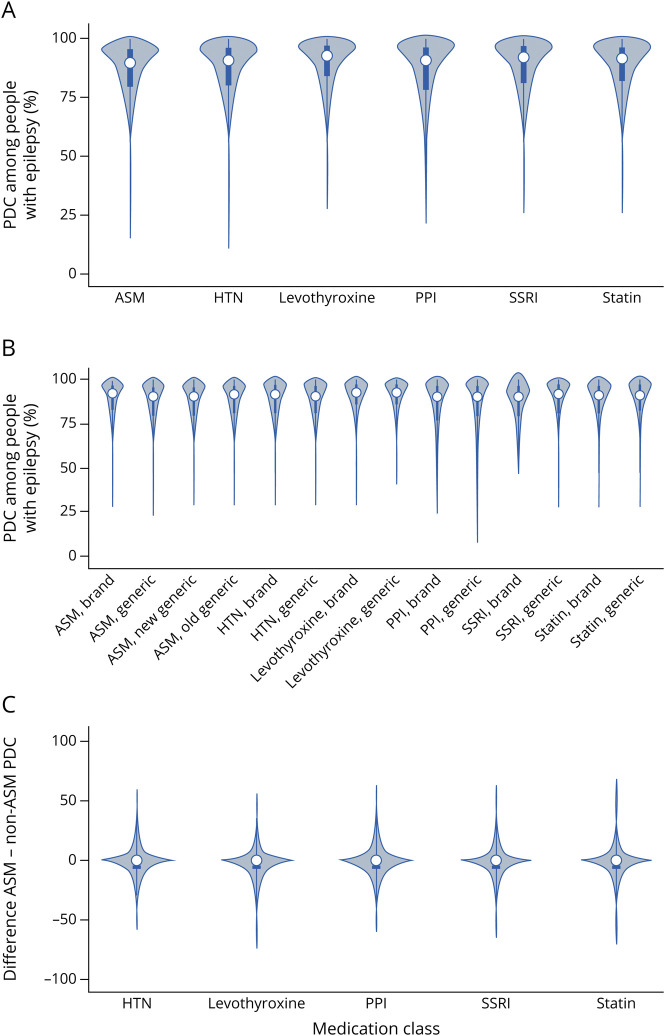
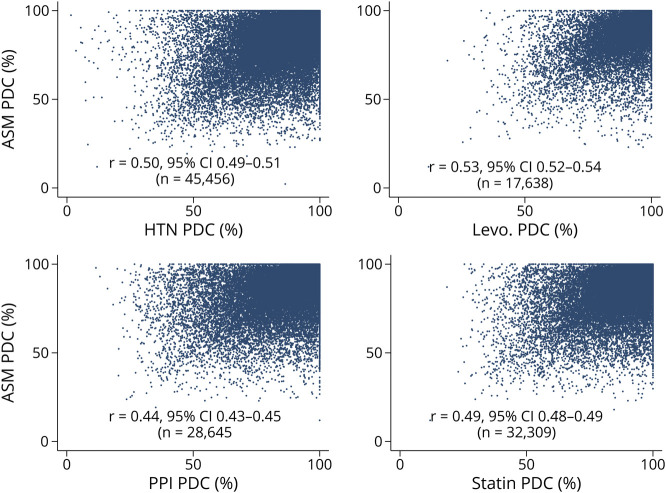
Results: There were 83,819 beneficiaries with epilepsy. Spearman correlation coefficients between ASM PDCs and each of the 5 non-ASM PDCs ranged from 0.44 to 0.50; Cohen κ ranged from 0.33 to 0.38; and within-person differences between the PDC of each ASM minus the PDC of each non-ASM were all statistically significant (p < 0.01), although median differences were all very close to 0. Fifty-four percent of variation in adherence across medications was due to differences between individuals. Adjusted predicted probabilities of adherence were as follows: ASMs 74% (95% confidence interval [CI] 73%-74%), proton pump inhibitors 74% (95% CI 74%-74%), antihypertensives 77% (95% CI 77%-78%), selective serotonin reuptake inhibitors 77% (95% CI 77%-78%), statins 78% (95% CI 78%-79%), and levothyroxine 82% (95% CI 81%-82%). Adjusted predicted probabilities of adherence to non-ASMs were 80% (95% CI 80%-81%) for beneficiaries with epilepsy vs 77% (95% CI 77%-77%) for beneficiaries without epilepsy.
Discussion: Among individuals with epilepsy, ASM adherence and non-ASM adherence were moderately correlated, half of the variation in adherence was due to between-person rather than between-medication differences, adjusted adherence was slightly lower for ASMs than several non-ASMs, and epilepsy was associated with a quite small increase in adherence to non-ASMs. Nonadherence to ASMs may provide an important cue to the clinician to inquire about adherence to other potentially life-prolonging medications as well. Although efforts should focus on improving ASM adherence, patient-level rather than purely medication-specific behaviors are also critical to consider when developing interventions to optimize adherence.
© 2021 American Academy of Neurology.
Figures
References
-
- Faught E. Adherence to antiepilepsy drug therapy. Epilepsy Behav. 2012;25(3):297-302. - PubMed
-
- Faught E, Duh MS, Weiner JR, Guérin A, Cunnington MC. Nonadherence to antiepileptic drugs and increased mortality: findings from the RANSOM study. Neurology. 2008;71(20):1572-1578. - PubMed
-
- Faught RE, Weiner JR, Guérin A, Cunnington MC, Duh MS. Impact of nonadherence to antiepileptic drugs on health care utilization and costs: findings from the RANSOM study. Epilepsia. 2009;50(3):501-509. - PubMed
-
- Ettinger AB, Manjunath R, Candrilli SD, Davis KL. Prevalence and cost of nonadherence to antiepileptic drugs in elderly patients with epilepsy. Epilepsy Behav. 2009;14(2):324-329. - PubMed