

Trends in neonatal intensive care unit admissions by race/ethnicity in the United States, 2008-2018
- PMID: 34893675
- PMCID: PMC8664880
- DOI: 10.1038/s41598-021-03183-1
Trends in neonatal intensive care unit admissions by race/ethnicity in the United States, 2008-2018
Abstract
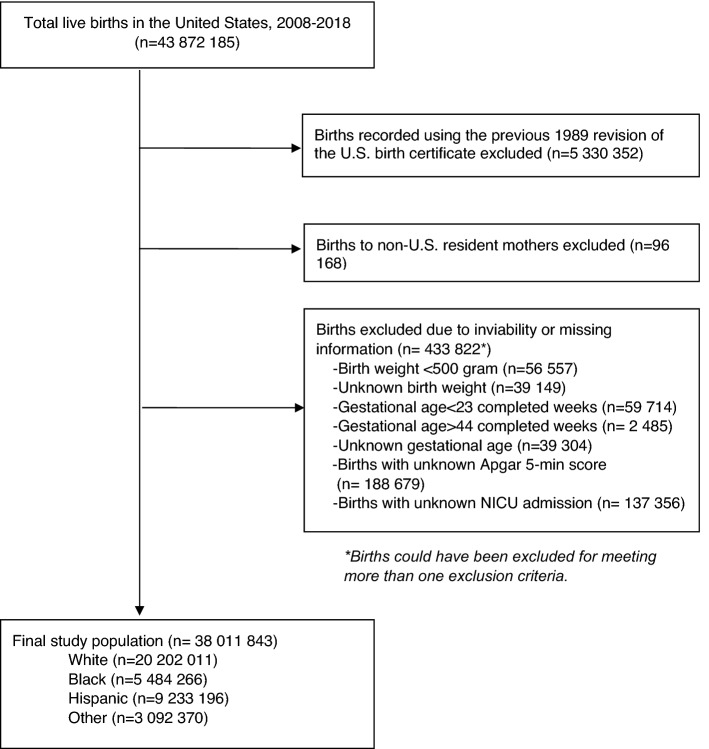
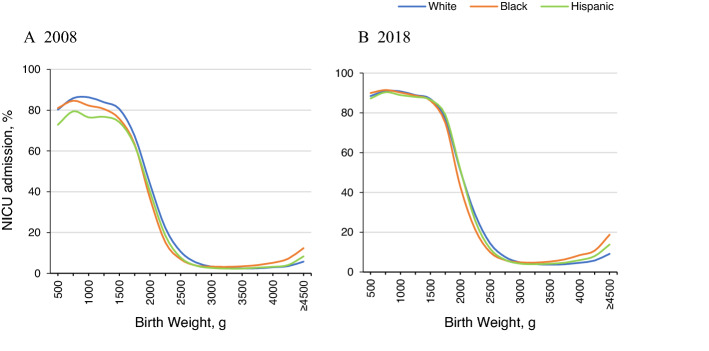
To examine temporal trends of NICU admissions in the U.S. by race/ethnicity, we conducted a retrospective cohort analysis using natality files provided by the National Center for Health Statistics at the U.S. Centers for Disease Control and Prevention. A total of 38,011,843 births in 2008-2018 were included. Crude and risk-adjusted NICU admission rates, overall and stratified by birth weight group, were compared between white, black, and Hispanic infants. Crude NICU admission rates increased from 6.62% (95% CI 6.59-6.65) to 9.07% (95% CI 9.04-9.10) between 2008 and 2018. The largest percentage increase was observed among Hispanic infants (51.4%) compared to white (29.1%) and black (32.4%) infants. Overall risk-adjusted rates differed little by race/ethnicity, but birth weight-stratified analysis revealed that racial/ethnic differences diminished in the very low birth weight (< 1500 g) and moderately low birth weight (1500-2499 g) groups. Overall NICU admission rates increased by 37% from 2008 to 2018, and the increasing trends were observed among all racial and ethnic groups. Diminished racial/ethnic differences in NICU admission rates in very low birth weight infants may reflect improved access to timely appropriate NICU care among high-risk infants through increasing health care coverage coupled with growing NICU supply.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Richardson DK, Reed K, Cutler JC, et al. Perinatal regionalization versus hospital competition: The Hartford example. Pediatrics. 1995;96:417–423. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
