

Impact of the COVID-19 Pandemic on Treatment Patterns for Patients With Metastatic Solid Cancer in the United States
- PMID: 34893865
- PMCID: PMC9002283
- DOI: 10.1093/jnci/djab225
Impact of the COVID-19 Pandemic on Treatment Patterns for Patients With Metastatic Solid Cancer in the United States
Abstract
Background: The COVID-19 pandemic has led to delays in patients seeking care for life-threatening conditions; however, its impact on treatment patterns for patients with metastatic cancer is unknown. We assessed the COVID-19 pandemic's impact on time to treatment initiation (TTI) and treatment selection for patients newly diagnosed with metastatic solid cancer.
Methods: We used an electronic health record-derived longitudinal database curated via technology-enabled abstraction to identify 14 136 US patients newly diagnosed with de novo or recurrent metastatic solid cancer between January 1 and July 31 in 2019 or 2020. Patients received care at approximately 280 predominantly community-based oncology practices. Controlled interrupted time series analyses assessed the impact of the COVID-19 pandemic period (April-July 2020) on TTI, defined as the number of days from metastatic diagnosis to receipt of first-line systemic therapy, and use of myelosuppressive therapy.
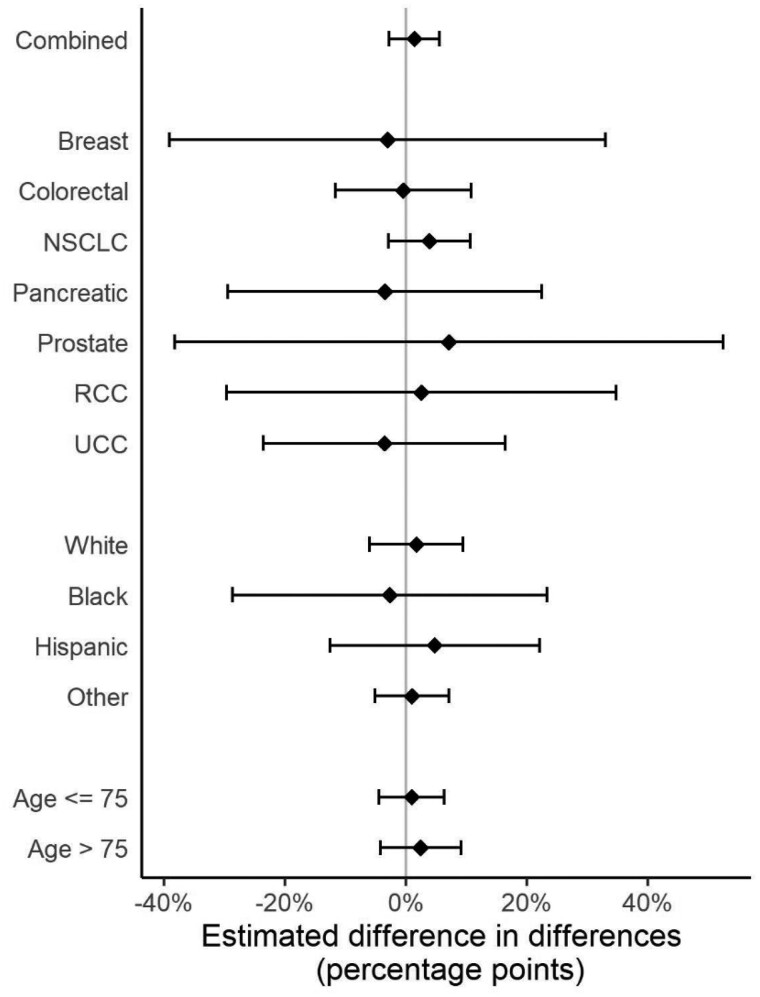
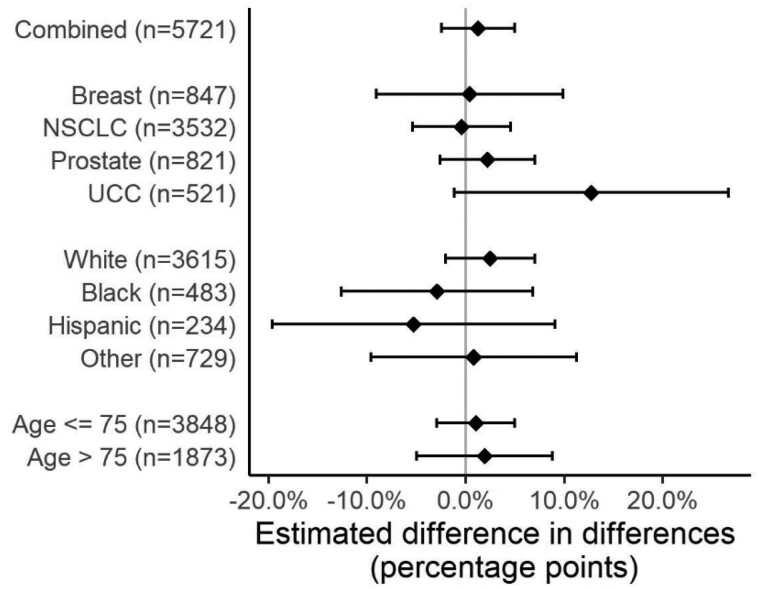
Results: The adjusted probability of treatment within 30 days of diagnosis was similar across periods (January-March 2019 = 41.7%, 95% confidence interval [CI] = 32.2% to 51.1%; April-July 2019 = 42.6%, 95% CI = 32.4% to 52.7%; January-March 2020 = 44.5%, 95% CI = 30.4% to 58.6%; April-July 2020 = 46.8%, 95% CI= 34.6% to 59.0%; adjusted percentage-point difference-in-differences = 1.4%, 95% CI = -2.7% to 5.5%). Among 5962 patients who received first-line systemic therapy, there was no association between the pandemic period and use of myelosuppressive therapy (adjusted percentage-point difference-in-differences = 1.6%, 95% CI = -2.6% to 5.8%). There was no meaningful effect modification by cancer type, race, or age.
Conclusions: Despite known pandemic-related delays in surveillance and diagnosis, the COVID-19 pandemic did not affect TTI or treatment selection for patients with metastatic solid cancers.
© The Author(s) 2021. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Update of
-
Impact of the COVID-19 pandemic on treatment patterns for US patients with metastatic solid cancer.medRxiv [Preprint]. 2021 Sep 23:2021.09.22.21263964. doi: 10.1101/2021.09.22.21263964. medRxiv. 2021. Update in: J Natl Cancer Inst. 2022 Apr 11;114(4):571-578. doi: 10.1093/jnci/djab225. PMID: 34611665 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
