

Monitoring for COVID-19 by universal testing in a homeless shelter in Germany: a prospective feasibility cohort study
- PMID: 34895157
- PMCID: PMC8665323
- DOI: 10.1186/s12879-021-06945-4
Monitoring for COVID-19 by universal testing in a homeless shelter in Germany: a prospective feasibility cohort study
Abstract
Background: Living conditions in homeless shelters facilitate the transmission of COVID-19. Social determinants and pre-existing health conditions place homeless people at increased risk of severe disease. Described outbreaks in homeless shelters resulted in high proportions of infected residents and staff members. In addition to other infection prevention strategies, regular shelter-wide (universal) testing for COVID-19 may be valuable, depending on the level of community transmission and when resources permit.
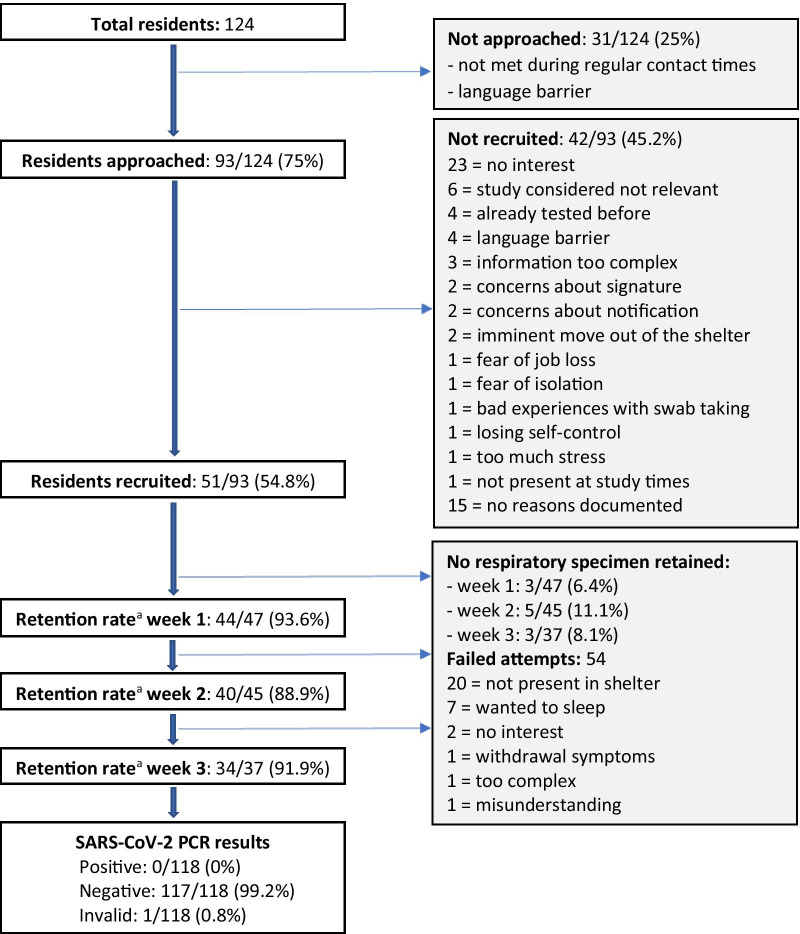
Methods: This was a prospective feasibility cohort study to evaluate universal testing for COVID-19 at a homeless shelter with 106 beds in Berlin, Germany. Co-researchers were recruited from the shelter staff. A PCR analysis of saliva or self-collected nasal/oral swab was performed weekly over a period of 3 weeks in July 2020. Acceptability and implementation barriers were analyzed by process evaluation using mixed methods including evaluation sheets, focus group discussion and a structured questionnaire.
Results: Ninety-three out of 124 (75%) residents were approached to participate in the study. Fifty-one out of the 93 residents (54.8%) gave written informed consent; thus 41.1% (51 out of 124) of all residents were included in the study. Among these, high retention rates (88.9-93.6%) of a weekly respiratory specimen were reached, but repeated collection attempts, as well as assistance were required. Around 48 person-hours were necessary for the sample collection including the preparation of materials. A self-collected nasal/oral swab was considered easier and more hygienic to collect than a saliva specimen. No resident was tested positive by RT-PCR. Language barriers were the main reason for non-participation. Flexibility of sample collection schedules, the use of video and audio materials, and concise written information were the main recommendations of the co-researchers for future implementation.
Conclusions: Voluntary universal testing for COVID-19 is feasible in homeless shelters. Universal testing of high-risk facilities will require flexible approaches, considering the level of the community transmission, the available resources, and the local recommendations. Lack of human resources and laboratory capacity may be a major barrier for implementation of universal testing, requiring adapted approaches compared to standard individual testing. Assisted self-collection of specimens and barrier free communication may facilitate implementation in homeless shelters. Program planning must consider homeless people's needs and life situation, and guarantee confidentiality and autonomy.
Keywords: COVID-19; Homeless shelter; Homelessness; Infection control; Monitoring; Pandemic; SARS-CoV-2.
© 2021. The Author(s).
Conflict of interest statement
TK reports having received honoraria outside of the topic of this study from Eli Lilly & Company, Teva, TotalEnergies, and The BMJ. All other authors have declared no conflicts of interest.
Figures
References
-
- Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, et al. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. Lancet. 2018;391(10117):241–50. doi: 10.1016/S0140-6736(17)31869-X. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
