

Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both idiopathic pulmonary fibrosis (IPF) and non-IPF: a systematic review and meta-analysis
- PMID: 34895203
- PMCID: PMC8666028
- DOI: 10.1186/s12890-021-01783-1
Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both idiopathic pulmonary fibrosis (IPF) and non-IPF: a systematic review and meta-analysis
Abstract
Background: Research questions To compare the efficacy of nintedanib and pirfenidone in the treatment of progressive pulmonary fibrosis; and to compare the efficacy of anti-fibrotic therapy (grouping nintedanib and pirfenidone together) in patients with IPF versus patients with progressive lung fibrosis not classified as IPF.
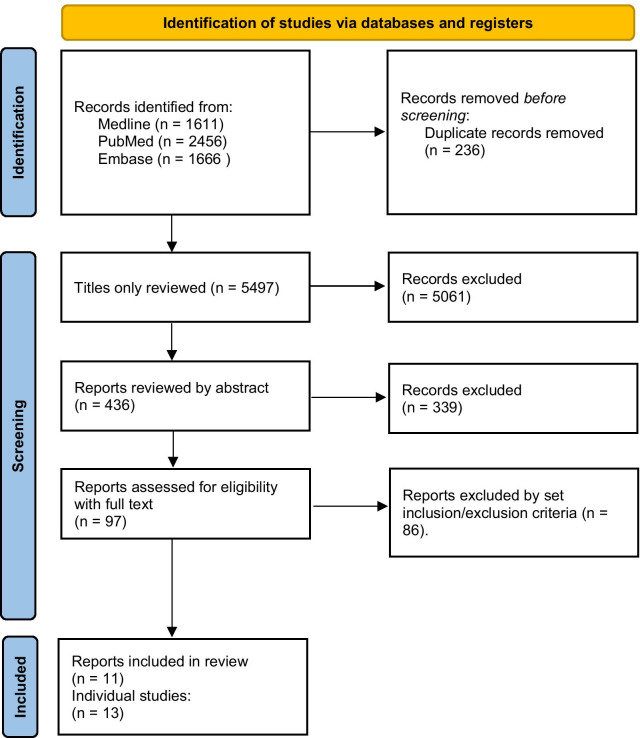
Study design and methods: A search of databases including MEDLINE, EMBASE, PubMed, and clinicaltrials.gov was conducted. Studies were included if they were randomised controlled trials of pirfenidone or nintedanib in adult patients with IPF or non-IPF patients, and with extractable data on mortality or decline in forced vital capacity (FVC). Random effects meta-analyses were performed on changes in FVC and where possible on mortality in the selected studies.
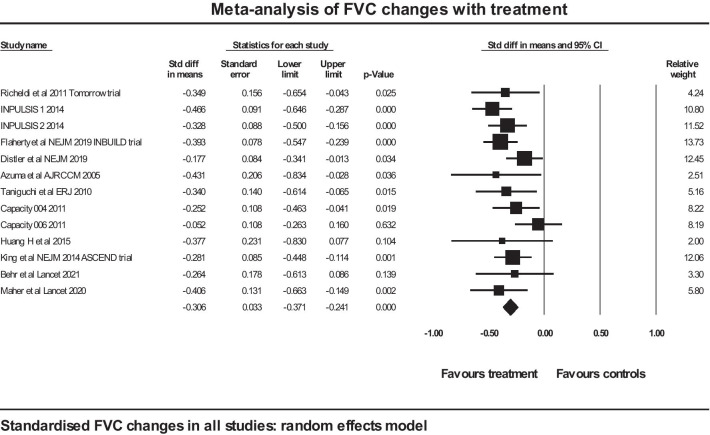
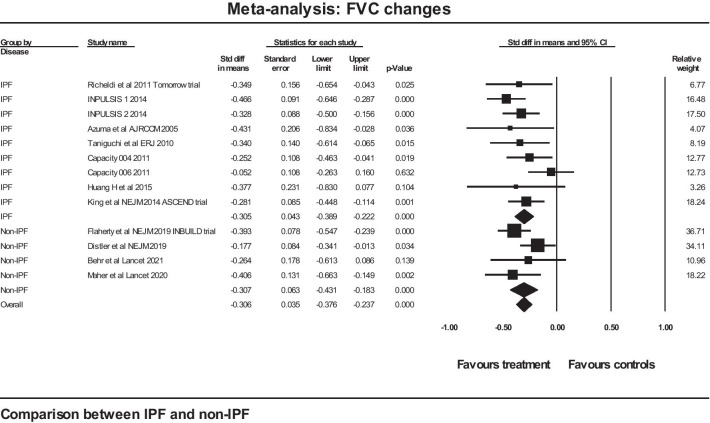
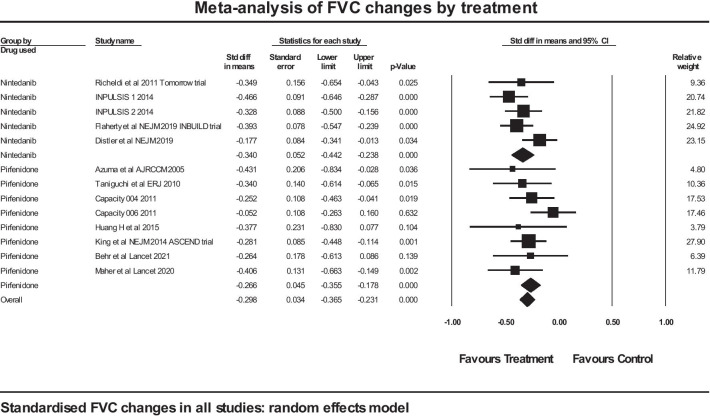
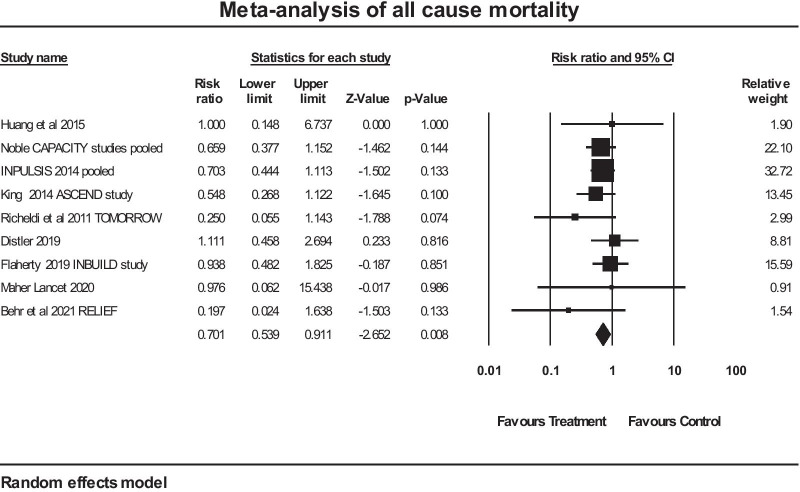
Results: 13 trials of antifibrotic therapy were pooled in a meta-analysis (with pirfenidone and nintedanib considered together as anti-fibrotic therapy). The change in FVC was expressed as a standardised difference to allow pooling of percentage and absolute changes. The mean effect size in the IPF studies was - 0.305 (SE 0.043) (p < 0.001) and in the non-IPF studies the figures were - 0.307 (SE 0.063) (p < 0.001). There was no evidence of any difference between the two groups for standardised rate of FVC decline (p = 0.979). Pooling IPF and non-IPF showed a significant reduction in mortality, with mean risk ratio of 07.01 in favour of antifibrotic therapy (p = 0.008). A separate analysis restricted to non-IPF did not show a significant reduction in mortality (risk ratio 0.908 (0.547 to 1.508), p = 0.71.
Interpretation: Anti-fibrotic therapy offers protection against the rate of decline in FVC in progressive lung fibrosis, with similar efficacy shown between the two anti-fibrotic agents currently in clinical use. There was no significant difference in efficacy of antifibrotic therapy whether the underlying condition was IPF or non-IPF with progressive fibrosis, supporting the hypothesis of a common pathogenesis. The data in this analysis was insufficient to be confident about a reduction in mortality in non-IPF with anti-fibrotic therapy. Trial Registration PROSPERO, registration number CRD42021266046.
Keywords: Idiopathic pulmonary fibrosis; Nintedanib; Pirfenidone.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have o conflicts of interest to disclose.
Figures
References
-
- National Institute for Health and Care Excellence. Idiopathic pulmonary fibrosis in adults: diagnosis and management [Internet] [London]: NICE; 2013 [updated 2017 May; cited 2021 Sept 27]. (Clinical guideline [CG163]). [Available from: https://www.nice.org.uk/guidance/cg163.
-
- National Institute for Health and Care Excellence. Pirfenidone for treating idiopathic pulmonary fibrosis [London]: NICE; 2018 [reviewed 2021 May; cited 2021 Sept 27]. (Technology appraisal guidance [TA504]). [Available from: https://www.nice.org.uk/guidance/ta504.
-
- National Institute for Health and Care Excellence. Nintedanib for treating idiopathic pulmonary fibrosis [London]: NICE; 2016 [cited 2021 Sept 27]. Technology appraisal guidance [TA379]) [Available from: https://www.nice.org.uk/guidance/ta379.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
