

Response-adapted omission of radiotherapy and comparison of consolidation chemotherapy in children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma (EuroNet-PHL-C1): a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial
- PMID: 34895479
- PMCID: PMC8716340
- DOI: 10.1016/S1470-2045(21)00470-8
Response-adapted omission of radiotherapy and comparison of consolidation chemotherapy in children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma (EuroNet-PHL-C1): a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial
Erratum in
-
Correction to Lancet Oncol 2022; 23: 125-37.Lancet Oncol. 2022 Feb;23(2):e59. doi: 10.1016/S1470-2045(22)00029-8. Lancet Oncol. 2022. PMID: 35114129 Free PMC article. No abstract available.
Abstract
Background: Children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma achieve an event-free survival at 5 years of about 90% after treatment with vincristine, etoposide, prednisone, and doxorubicin (OEPA) followed by cyclophosphamide, vincristine, prednisone, and procarbazine (COPP) and radiotherapy, but long-term treatment effects affect survival and quality of life. We aimed to investigate whether radiotherapy can be omitted in patients with morphological and metabolic adequate response to OEPA and whether modified consolidation chemotherapy reduces gonadotoxicity.
Methods: Our study was designed as a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial, and was carried out at 186 hospital sites across 16 European countries. Children and adolescents with newly diagnosed intermediate-stage (treatment group 2) and advanced-stage (treatment group 3) classical Hodgkin lymphoma who were younger than 18 years and stratified according to risk using Ann Arbor disease stages IIAE, IIB, IIBE, IIIA, IIIAE, IIIB, IIIBE, and all stages IV (A, B, AE, and BE) were included in the study. Patients with early disease (treatment group 1) were excluded from this analysis. All patients were treated with two cycles of OEPA (1·5 mg/m2 vincristine taken intravenously capped at 2 mg, on days 1, 8, and 15; 125 mg/m2 etoposide taken intravenously on days 1-5; 60 mg/m2 prednisone taken orally on days 1-15; and 40 mg/m2 doxorubicin taken intravenously on days 1 and 15). Patients were randomly assigned to two (treatment group 2) or four (treatment group 3) cycles of COPP (500 mg/m2 cyclophosphamide taken intravenously on days 1 and 8; 1·5 mg/m2 vincristine taken intravenously capped at 2 mg, on days 1 and 8; 40 mg/m2 prednisone taken orally on days 1 to 15; and 100 mg/m2 procarbazine taken orally on days 1 to 15) or COPDAC, which was identical to COPP except that 250 mg/m2 dacarbazine administered intravenously on days 1 to 3 replaced procarbazine. The method of randomisation (1:1) was minimisation with stochastic component and was centrally stratified by treatment group, country, trial sites, and sex. The primary endpoint was event-free survival, defined as time from treatment start until the first of the following events: death from any cause, progression or relapse of classical Hodgkin lymphoma, or occurrence of secondary malignancy. The primary objectives were maintaining 90% event-free survival at 5 years in patients with adequate response to OEPA treated without radiotherapy and to exclude a decrease of 8% in event-free survival at 5 years in the embedded COPDAC versus COPP randomisation to show non-inferiority of COPDAC. Efficacy analyses are reported per protocol and safety in the intention-to-treat population. The trial is registered with ClinicalTrials.gov (trial number NCT00433459) and EUDRACT (trial number 2006-000995-33), and is closed to recruitment.
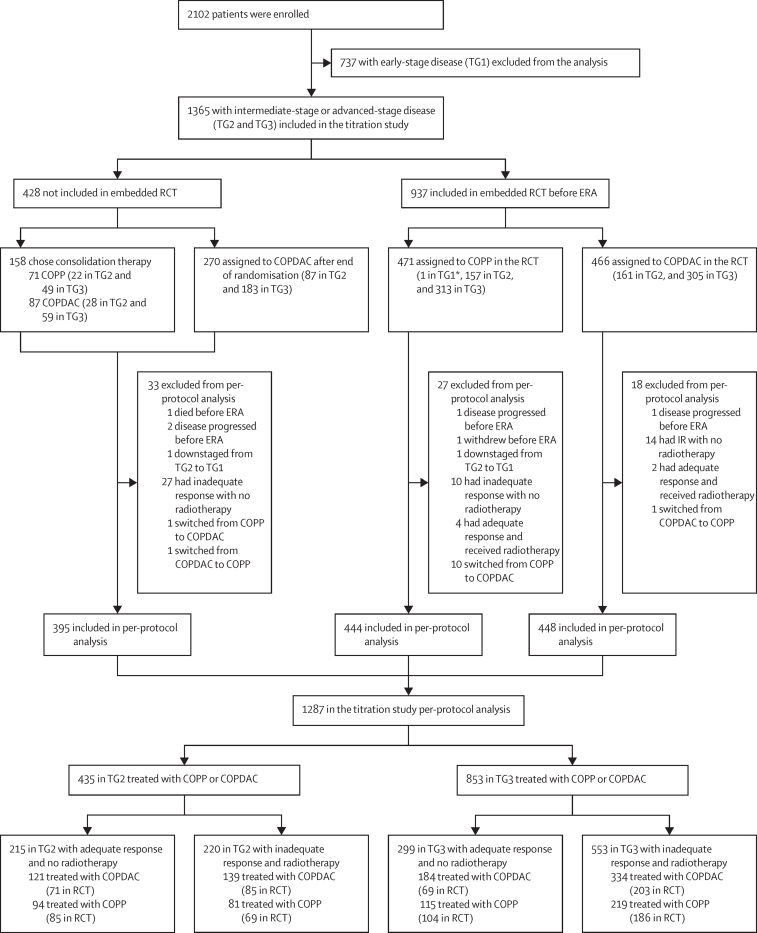
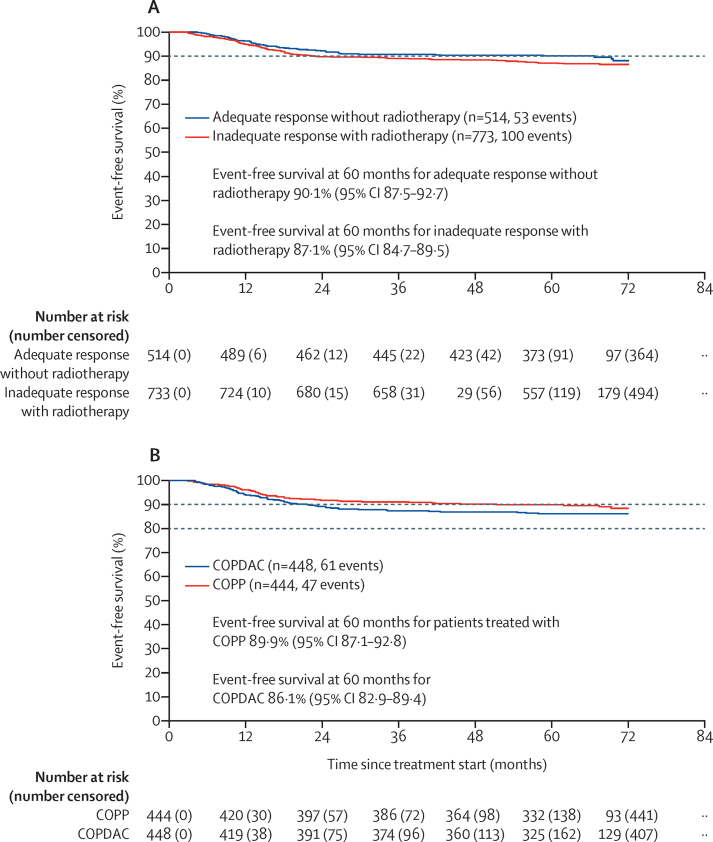
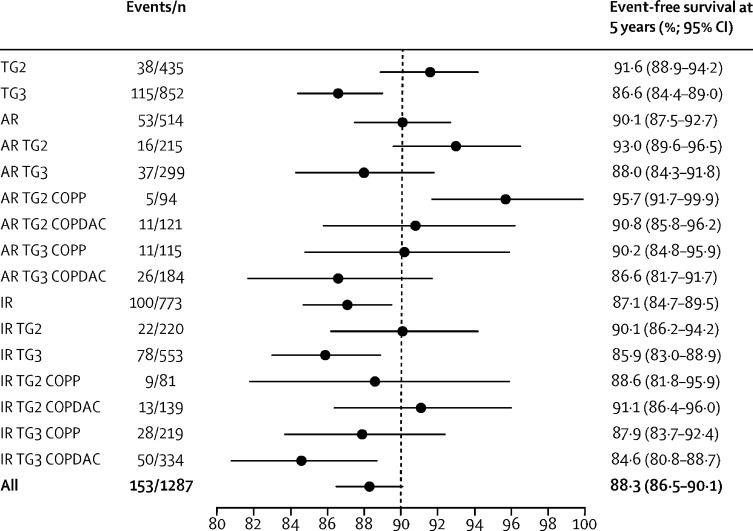
Findings: Between Jan 31, 2007, and Jan 30, 2013, 2102 patients were recruited. 737 (35%) of the 2102 recruited patients were in treatment group 1 (early-stage disease) and were not included in our analysis. 1365 (65%) of the 2102 patients were in treatment group 2 (intermediate-stage disease; n=455) and treatment group 3 (advanced-stage disease; n=910). Of these 1365, 1287 (94%) patients (435 [34%] of 1287 in treatment group 2 and 852 [66%] of 1287 in treatment group 3) were included in the titration trial per-protocol analysis. 937 (69%) of 1365 patients were randomly assigned to COPP (n=471) or COPDAC (n=466) in the embedded trial. Median follow-up was 66·5 months (IQR 62·7-71·7). Of 1287 patients in the per-protocol group, 514 (40%) had an adequate response to treatment and were not treated with radiotherapy (215 [49%] of 435 in treatment group 2 and 299 [35%] of 852 in treatment group 3). 773 (60%) of 1287 patients with inadequate response were scheduled for radiotherapy (220 [51%] of 435 in the treatment group 2 and 553 [65%] of 852 in treatment group 3. In patients who responded adequately, event-free survival rates at 5 years were 90·1% (95% CI 87·5-92·7). event-free survival rates at 5 years in 892 patients who were randomly assigned to treatment and analysed per protocol were 89·9% (95% CI 87·1-92·8) for COPP (n=444) versus 86·1% (82·9-89·4) for COPDAC (n=448). The COPDAC minus COPP difference in event-free survival at 5 years was -3·7% (-8·0 to 0·6). The most common grade 3-4 adverse events (intention-to-treat population) were decreased haemoglobin (205 [15%] of 1365 patients during OEPA vs 37 [7%] of 528 treated with COPP vs 20 [2%] of 819 treated with COPDAC), decreased white blood cells (815 [60%] vs 231 [44%] vs 84 [10%]), and decreased neutrophils (1160 [85%] vs 223 [42%] vs 174 [21%]). One patient in treatment group 2 died of sepsis after the first cycle of OEPA; no other treatment-related deaths occurred.
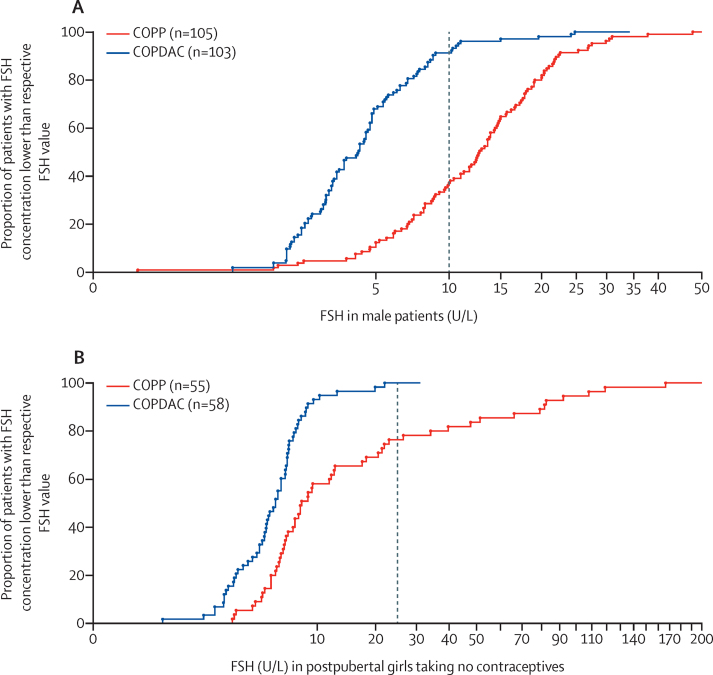
Interpretation: Our results show that radiotherapy can be omitted in patients who adequately respond to treatment, when consolidated with COPP or COPDAC. COPDAC might be less effective, but is substantially less gonadotoxic than COPP. A high proportion of patients could therefore be spared radiotherapy, eventually reducing the late effects of treatment. With more refined criteria for response assessment, the number of patients who receive radiotherapy will be further decreased.
Funding: Deutsche Krebshilfe, Elternverein für Krebs-und leukämiekranke Kinder Gießen, Kinderkrebsstiftung Mainz, Tour der Hoffnung, Menschen für Kinder, Programme Hospitalier de Recherche Clinique, and Cancer Research UK.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
All eyes on the EuroNet-PHL-C1 trial for paediatric classical Hodgkin lymphoma.Lancet Oncol. 2022 Jan;23(1):11-13. doi: 10.1016/S1470-2045(21)00544-1. Epub 2021 Dec 9. Lancet Oncol. 2022. PMID: 34895480 No abstract available.
-
[Omission of radiotherapy depending on treatment response in children and adolescents with intermediate-stage and advanced-stage Hodgkin lymphoma. Comparison with other consolidation therapies (EuroNet-PHL-C1): a titration study].Strahlenther Onkol. 2022 Jun;198(6):593-594. doi: 10.1007/s00066-022-01923-4. Epub 2022 Apr 1. Strahlenther Onkol. 2022. PMID: 35364689 Free PMC article. German. No abstract available.
References
-
- Schellong G, Bramswig J, Ludwig R, et al. Combined treatment strategy in over 200 children with Hodgkin's disease: graduated chemotherapy, involved field irradiation with low dosage and selective splenectomy. A report of the cooperative therapy study DAL-HD-82. Klin Padiatr. 1986;198:137–146. - PubMed
-
- Schellong G, Potter R, Bramswig J, et al. High cure rates and reduced long-term toxicity in pediatric Hodgkin's disease: the German-Austrian multicenter trial DAL-HD-90. The German-Austrian Pediatric Hodgkin's Disease Study Group. J Clin Oncol. 1999;17:3736–3744. - PubMed
-
- Weiner MA, Leventhal B, Brecher ML, et al. Randomized study of intensive MOPP-ABVD with or without low-dose total-nodal radiation therapy in the treatment of stages IIB, IIIA2, IIIB, and IV Hodgkin's disease in pediatric patients: a Pediatric Oncology Group study. J Clin Oncol. 1997;15:2769–2779. - PubMed
-
- Donaldson SS, Hudson MM, Lamborn KR, et al. VAMP and low-dose, involved-field radiation for children and adolescents with favorable, early-stage Hodgkin's disease: results of a prospective clinical trial. J Clin Oncol. 2002;20:3081–3087. - PubMed
