

Using multivariable Mendelian randomization to estimate the causal effect of bone mineral density on osteoarthritis risk, independently of body mass index
- PMID: 34897459
- PMCID: PMC9365636
- DOI: 10.1093/ije/dyab251
Using multivariable Mendelian randomization to estimate the causal effect of bone mineral density on osteoarthritis risk, independently of body mass index
Abstract
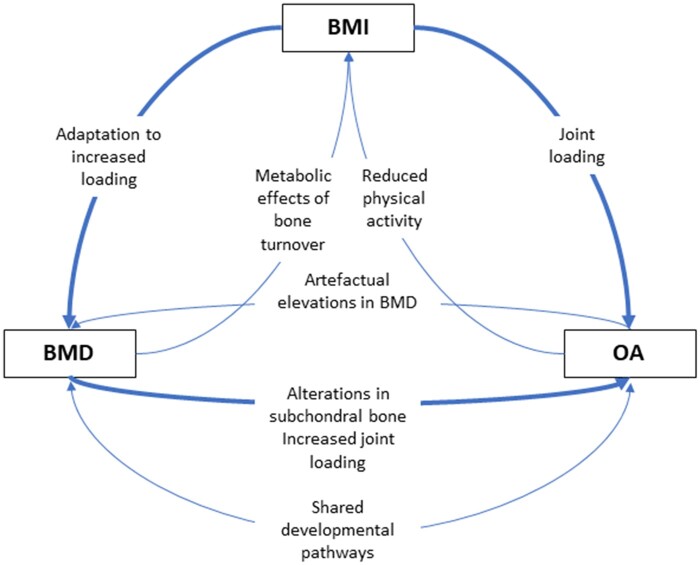
Objectives: Observational analyses suggest that high bone mineral density (BMD) is a risk factor for osteoarthritis (OA); it is unclear whether this represents a causal effect or shared aetiology and whether these relationships are body mass index (BMI)-independent. We performed bidirectional Mendelian randomization (MR) to uncover the causal pathways between BMD, BMI and OA.
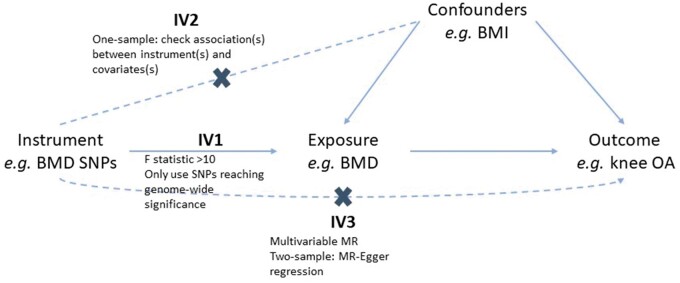
Methods: One-sample (1S)MR estimates were generated by two-stage least-squares regression. Unweighted allele scores instrumented each exposure. Two-sample (2S)MR estimates were generated using inverse-variance weighted random-effects meta-analysis. Multivariable MR (MVMR), including BMD and BMI instruments in the same model, determined the BMI-independent causal pathway from BMD to OA. Latent causal variable (LCV) analysis, using weight-adjusted femoral neck (FN)-BMD and hip/knee OA summary statistics, determined whether genetic correlation explained the causal effect of BMD on OA.
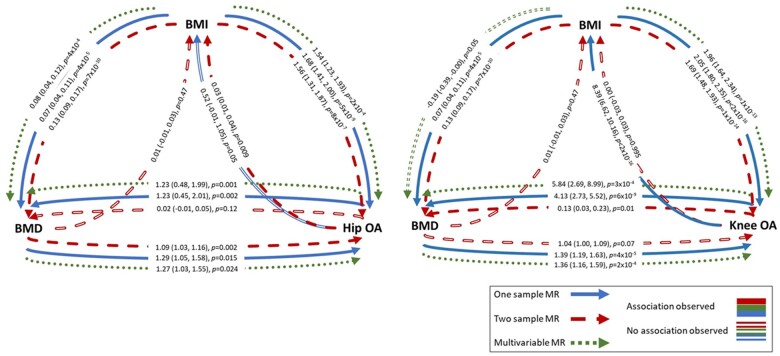
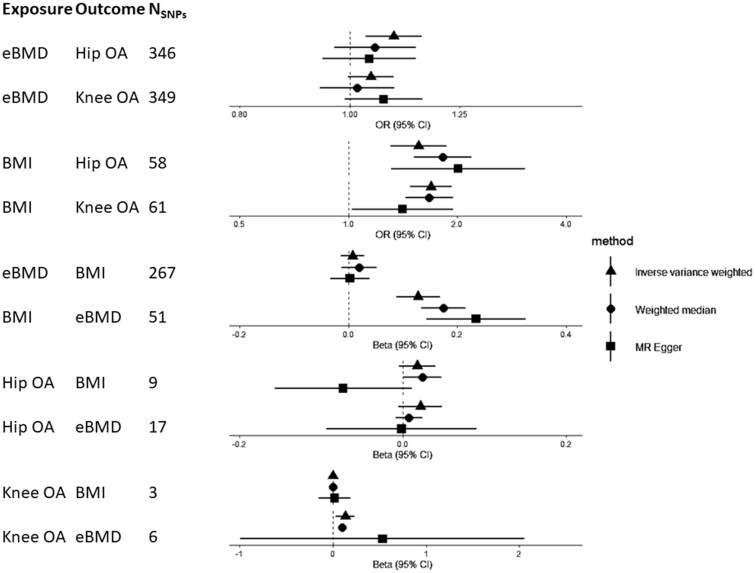
Results: 1SMR provided strong evidence for a causal effect of BMD estimated from heel ultrasound (eBMD) on hip and knee OA {odds ratio [OR]hip = 1.28 [95% confidence interval (CI) = 1.05, 1.57], p = 0.02, ORknee = 1.40 [95% CI = 1.20, 1.63], p = 3 × 10-5, OR per standard deviation [SD] increase}. 2SMR effect sizes were consistent in direction. Results suggested that the causal pathways between eBMD and OA were bidirectional (βhip = 1.10 [95% CI = 0.36, 1.84], p = 0.003, βknee = 4.16 [95% CI = 2.74, 5.57], p = 8 × 10-9, β = SD increase per doubling in risk). MVMR identified a BMI-independent causal pathway between eBMD and hip/knee OA. LCV suggested that genetic correlation (i.e. shared genetic aetiology) did not fully explain the causal effects of BMD on hip/knee OA.
Conclusions: These results provide evidence for a BMI-independent causal effect of eBMD on OA. Despite evidence of bidirectional effects, the effect of BMD on OA did not appear to be fully explained by shared genetic aetiology, suggesting a direct action of bone on joint deterioration.
Keywords: Mendelian randomization; Osteoarthritis; UK Biobank; body mass index; bone mineral density.
© The Author(s) 2021. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Smith GD, Ebrahim S.. ‘Mendelian randomization’: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol 2003;32:1–22. - PubMed
-
- Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G.. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med 2008;27:1133–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
