

Sepsis prediction, early detection, and identification using clinical text for machine learning: a systematic review
- PMID: 34897469
- PMCID: PMC8800516
- DOI: 10.1093/jamia/ocab236
Sepsis prediction, early detection, and identification using clinical text for machine learning: a systematic review
Abstract
Objective: To determine the effects of using unstructured clinical text in machine learning (ML) for prediction, early detection, and identification of sepsis.
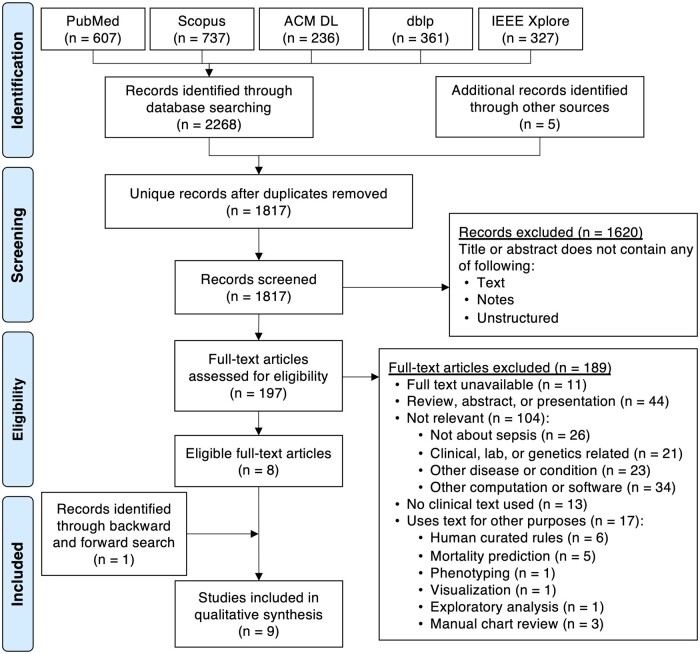
Materials and methods: PubMed, Scopus, ACM DL, dblp, and IEEE Xplore databases were searched. Articles utilizing clinical text for ML or natural language processing (NLP) to detect, identify, recognize, diagnose, or predict the onset, development, progress, or prognosis of systemic inflammatory response syndrome, sepsis, severe sepsis, or septic shock were included. Sepsis definition, dataset, types of data, ML models, NLP techniques, and evaluation metrics were extracted.
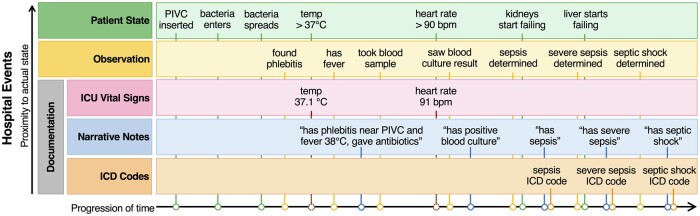
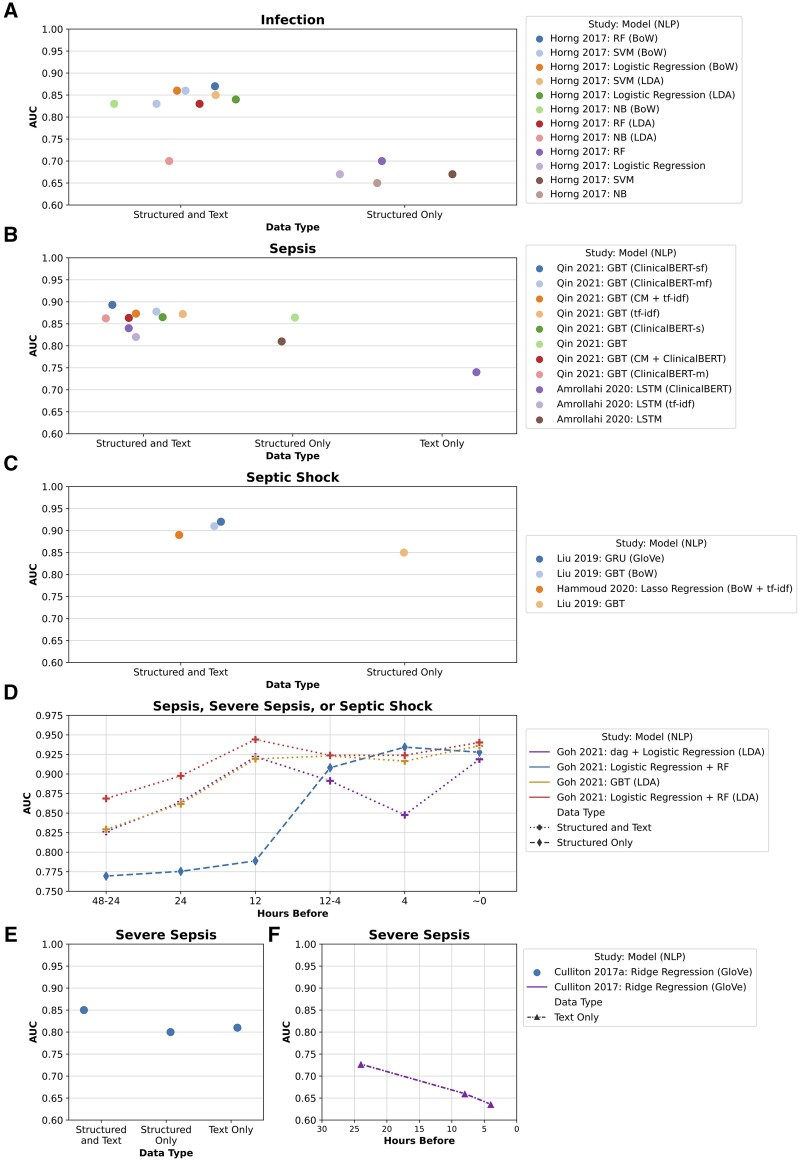
Results: The clinical text used in models include narrative notes written by nurses, physicians, and specialists in varying situations. This is often combined with common structured data such as demographics, vital signs, laboratory data, and medications. Area under the receiver operating characteristic curve (AUC) comparison of ML methods showed that utilizing both text and structured data predicts sepsis earlier and more accurately than structured data alone. No meta-analysis was performed because of incomparable measurements among the 9 included studies.
Discussion: Studies focused on sepsis identification or early detection before onset; no studies used patient histories beyond the current episode of care to predict sepsis. Sepsis definition affects reporting methods, outcomes, and results. Many methods rely on continuous vital sign measurements in intensive care, making them not easily transferable to general ward units.
Conclusions: Approaches were heterogeneous, but studies showed that utilizing both unstructured text and structured data in ML can improve identification and early detection of sepsis.
Keywords: electronic health records; machine learning; natural language processing; sepsis; systematic review.
© The Author(s) 2021. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NKJ, et al. ; International Forum of Acute Care Trialists. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med 2016; 193 (3): 259–72. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345 (19): 1368–77. - PubMed
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34: 1589–96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
