

Initial experience in staging primary oesophageal/gastro-oesophageal cancer with 18F-FDG PET/MRI
- PMID: 34897589
- PMCID: PMC8666393
- DOI: 10.1186/s41824-021-00117-y
Initial experience in staging primary oesophageal/gastro-oesophageal cancer with 18F-FDG PET/MRI
Abstract
Background: 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging (18F-FDG PET/MRI) may improve cancer staging by combining sensitive cancer detection with high-contrast resolution and detail. We compared the diagnostic performance of 18F-FDG PET/MRI to 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for staging oesophageal/gastro-oesophageal cancer. Following ethical approval and informed consent, participants with newly diagnosed primary oesophageal/gastro-oesophageal cancer were enrolled. Exclusions included prior/concurrent malignancy. Following 324 ± 28 MBq 18F-FDG administration and 60-min uptake, PET/CT was performed, immediately followed by integrated PET/MRI from skull base to mid-thigh. PET/CT was interpreted by two dual-accredited nuclear medicine physicians and PET/MRI by a dual-accredited nuclear medicine physician/radiologist and cancer radiologist in consensus. Per-participant staging was compared with the tumour board consensus staging using the McNemar test, with statistical significance at 5%.
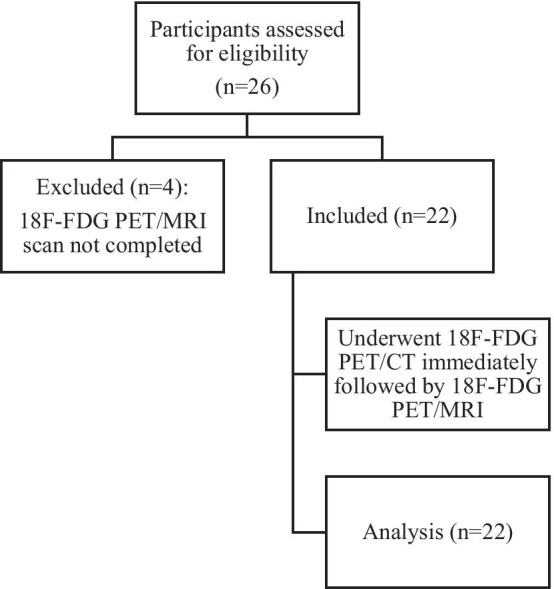
Results: Out of 26 participants, 22 (20 males; mean ± SD age 68.8 ± 8.7 years) completed 18F-FDG PET/CT and PET/MRI. Compared to the tumour board, the primary tumour was staged concordantly in 55% (12/22) with PET/MRI and 36% (8/22) with PET/CT; the nodal stage was concordant in 45% (10/22) with PET/MRI and 50% (11/22) with PET/CT. There was no statistical difference in PET/CT and PET/MRI staging performance (p > 0.05, for T and N staging). The staging of distant metastases was concordant with the tumour board in 95% (21/22) with both PET/MRI and PET/CT. Of participants with distant metastatic disease, PET/MRI detected additional metastases in 30% (3/10).
Conclusion: In this preliminary study, compared to 18F-FDG PET/CT, 18F-FDG PET/MRI showed non-significant higher concordance with T-staging, but no difference with N or M-staging. Additional metastases detected by 18F-FDG PET/MRI may be of additive clinical value.
Keywords: Gastro-oesophageal cancer; Oesophageal cancer; PET/CT; PET/MR.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources