

Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19: A systematic review and meta-analysis
- PMID: 34897631
- PMCID: PMC8890412
- DOI: 10.5603/CJ.a2021.0167
Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19: A systematic review and meta-analysis
Abstract
Background: Atrial fibrillation (AF) is the most common cardiac arrhythmia in the adult population. Herein, is a systematic review with meta-analysis to determine the impact of AF/atrial flutter (AFL) on mortality, as well as individual complications in patients hospitalized with the coronavirus disease 2019 (COVID-19).
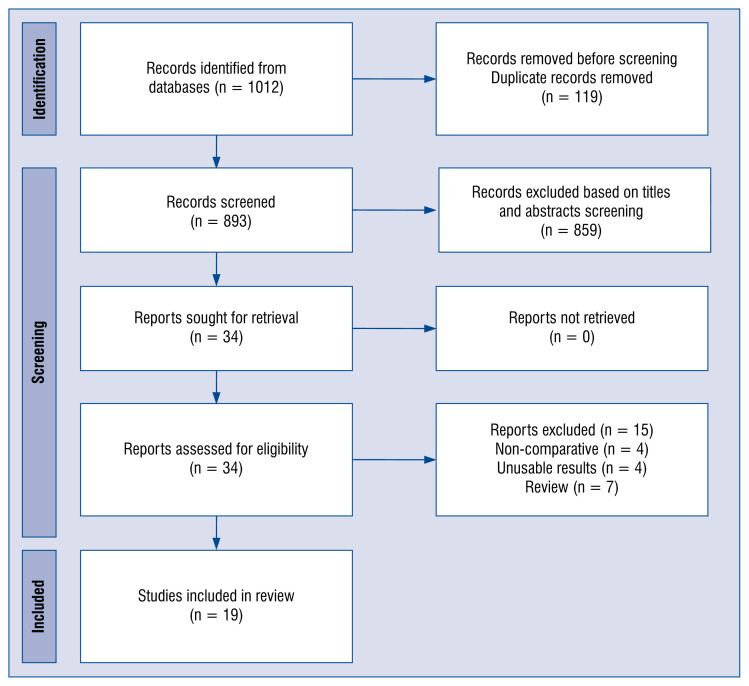
Methods: A systematic search of the SCOPUS, Medline, Web of Science, CINAHL and Cochrane databases was performed. The a priori primary outcome of interest was in-hospital mortality. A random-effects model was used to pool study results.
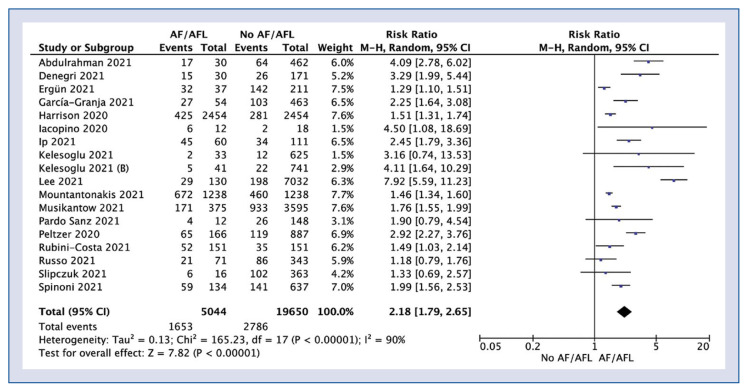
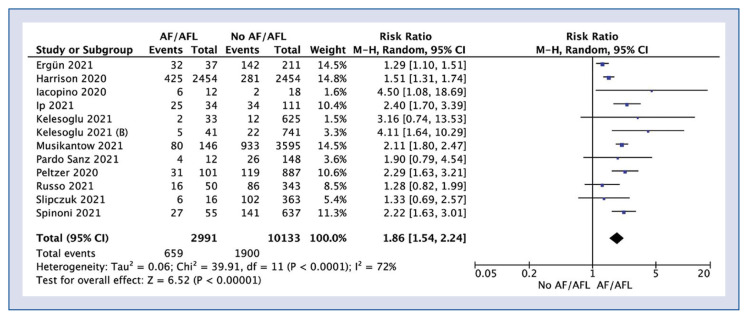
Results: Nineteen studies which included 33,296 patients were involved in this meta-analysis. Inhospital mortality for AF/AFL vs. no-AF/AFL groups varied and amounted to 32.8% vs. 14.2%, respectively (risk ratio [RR]: 2.18; 95% confidence interval [CI]: 1.79-2.65; p < 0.001). In-hospital mortality in new onset AF/AFL compared to no-AFAFL was 22.0% vs. 18.8% (RR: 1.86; 95% CI: 1.54-2.24; p < 0.001). Intensive care unit (ICU) admission was required for 17.7% of patients with AF/AFL compared to 10.8% for patients without AF/AFL (RR: 1.94; 95% CI: 1.04-3.62; p = 0.04).
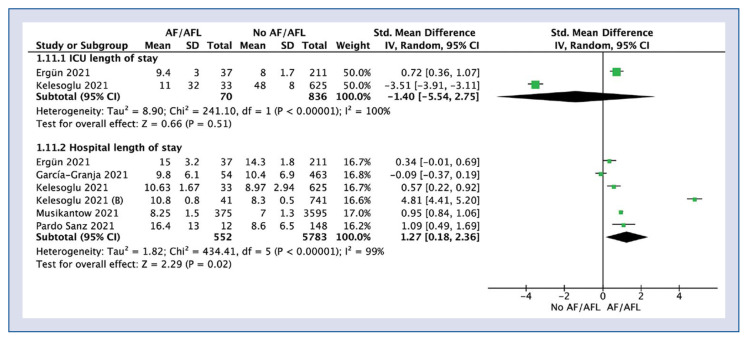
Conclusions: The present study reveals that AF/AFL is associated with increased in-hospital mortality and worse outcomes in patients with COVID-19 and may be used as a negative prognostic factor in these patients. Patients with AF/AFL are at higher risk of hospitalization in ICU. The presence of AF/AFL in individuals with COVID-19 is associated with higher risk of complications, such as bleeding, acute kidney injury and heart failure. AF/AFL may be associated with unfavorable outcomes due to the hemodynamic compromise of cardiac function itself or hyperinflammatory state typical of these conditions.
Keywords: COVID-19; atrial fibrillation; atrial flutter; meta-analysis; new onset atrial fibrillation; outcome; systematic review.
Conflict of interest statement
Figures
References
-
- Ruetzler K, Szarpak L, Filipiak K, et al. The COVID-19 pandemic — a view of the current state of the problem. Dis Emerg Med J. 2020 doi: 10.5603/demj.a2020.0015.. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
