

Exercise-Induced Cardiac Troponin Elevations: From Underlying Mechanisms to Clinical Relevance
- PMID: 34898243
- PMCID: PMC8663527
- DOI: 10.1161/CIRCULATIONAHA.121.056208
Exercise-Induced Cardiac Troponin Elevations: From Underlying Mechanisms to Clinical Relevance
Abstract
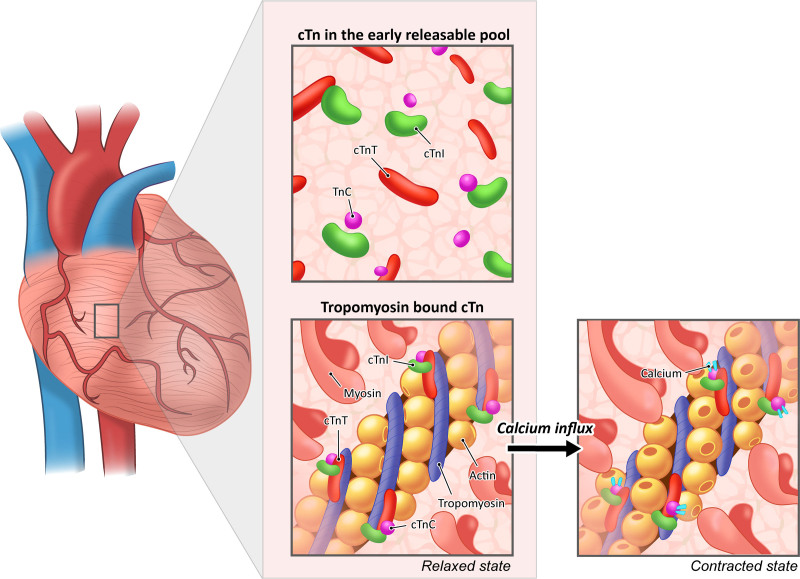
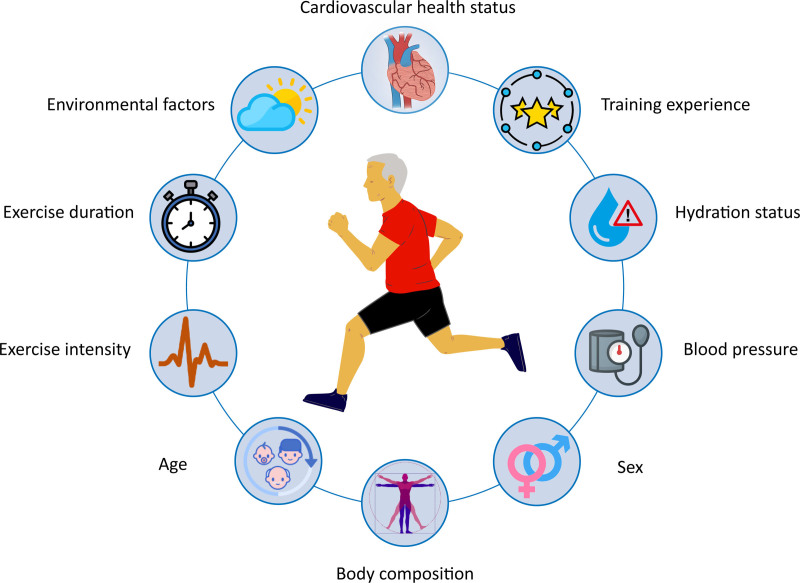
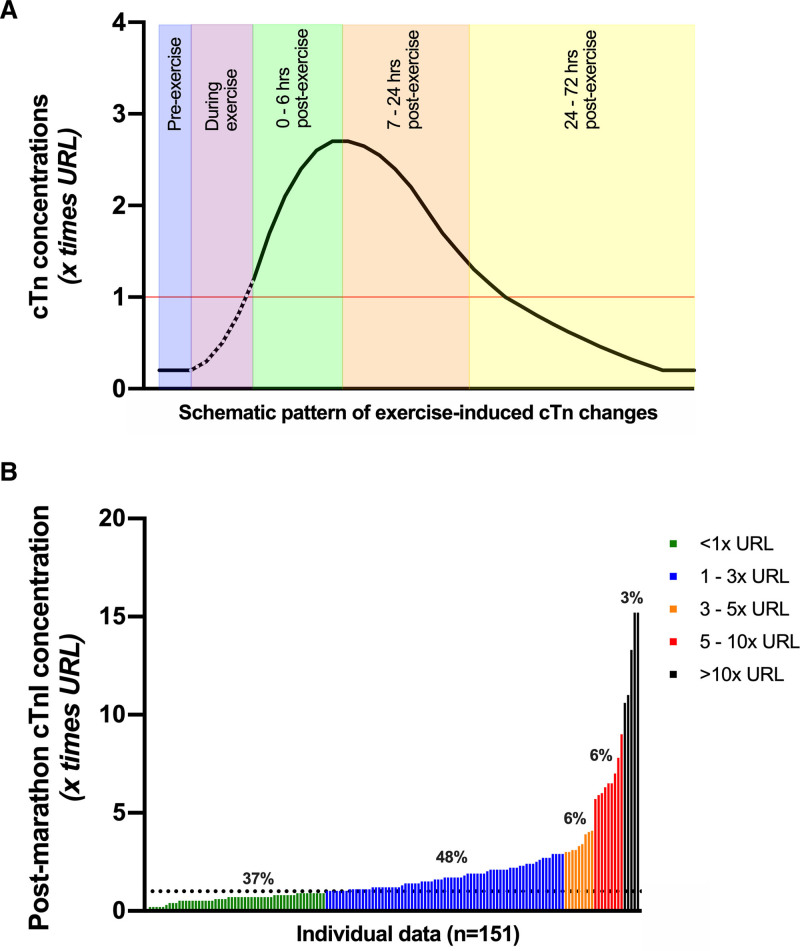
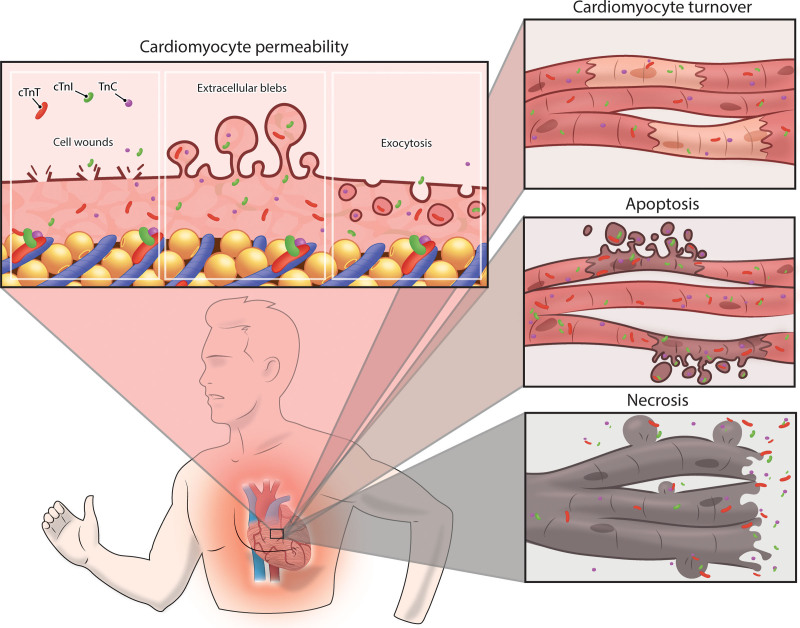
Serological assessment of cardiac troponins (cTn) is the gold standard to assess myocardial injury in clinical practice. A greater magnitude of acutely or chronically elevated cTn concentrations is associated with lower event-free survival in patients and the general population. Exercise training is known to improve cardiovascular function and promote longevity, but exercise can produce an acute rise in cTn concentrations, which may exceed the upper reference limit in a substantial number of individuals. Whether exercise-induced cTn elevations are attributable to a physiological or pathological response and if they are clinically relevant has been debated for decades. Thus far, exercise-induced cTn elevations have been viewed as the only benign form of cTn elevations. However, recent studies report intriguing findings that shed new light on the underlying mechanisms and clinical relevance of exercise-induced cTn elevations. We will review the biochemical characteristics of cTn assays, key factors determining the magnitude of postexercise cTn concentrations, the release kinetics, underlying mechanisms causing and contributing to exercise-induced cTn release, and the clinical relevance of exercise-induced cTn elevations. We will also explain the association with cardiac function, correlates with (subclinical) cardiovascular diseases and exercise-induced cTn elevations predictive value for future cardiovascular events. Last, we will provide recommendations for interpretation of these findings and provide direction for future research in this field.
Keywords: apoptosis; athletes; cardiomegaly, exercise-induced; heart; heart injuries; necrosis.
Figures
References
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018; 138:e618–e651. doi: 10.1161/CIR.0000000000000617 - PubMed
-
- Eggers KM, Jernberg T, Lindahl B. Cardiac troponin elevation in patients without a specific diagnosis. J Am Coll Cardiol. 2019; 73:1–9. doi: 10.1016/j.jacc.2018.09.082 - PubMed
-
- Roos A, Bandstein N, Lundbäck M, Hammarsten O, Ljung R, Holzmann MJ. Stable high-sensitivity cardiac troponin T levels and outcomes in patients with chest pain. J Am Coll Cardiol. 2017; 70:2226–2236. doi: 10.1016/j.jacc.2017.08.064 - PubMed
-
- Sze J, Mooney J, Barzi F, Hillis GS, Chow CK. Cardiac troponin and its relationship to cardiovascular outcomes in community populations: a systematic review and meta-analysis. Heart Lung Circ. 2016; 25:217–228. doi: 10.1016/j.hlc.2015.09.001 - PubMed
-
- Shave R, Baggish A, George K, Wood M, Scharhag J, Whyte G, Gaze D, Thompson PD. Exercise-induced cardiac troponin elevation: evidence, mechanisms, and implications. J Am Coll Cardiol. 2010; 56:169–176. doi: 10.1016/j.jacc.2010.03.037 - PubMed
