

Clinical Phenotype of Cerebral Palsy Depends on the Cause: Is It Really Cerebral Palsy? A Retrospective Study
- PMID: 34898314
- PMCID: PMC8804944
- DOI: 10.1177/08830738211059686
Clinical Phenotype of Cerebral Palsy Depends on the Cause: Is It Really Cerebral Palsy? A Retrospective Study
Abstract
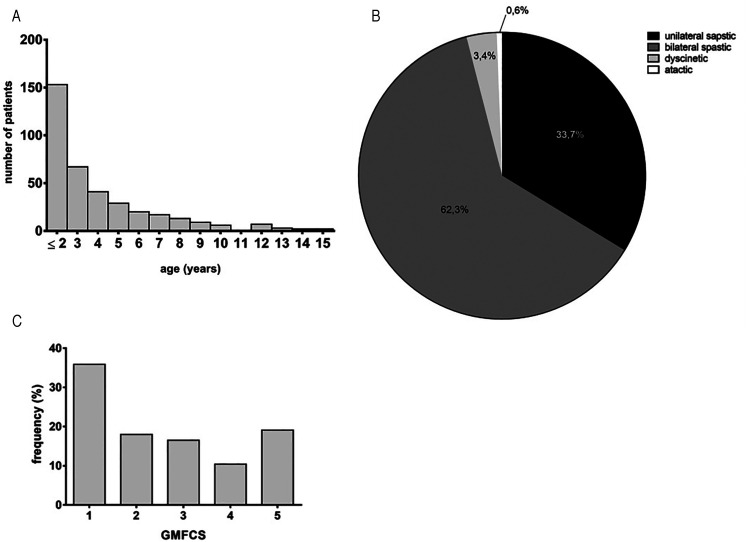
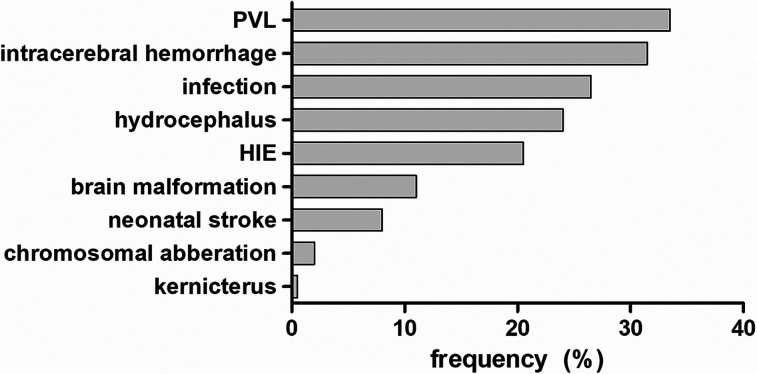
Cerebral palsy is the most common motor disability in childhood. Still, the precise definition in terms of causes and timing of the brain damage remains controversial. Several studies examine the clinical phenotype of cerebral palsy types. The aim of our study was to determine to what extent the clinical phenotype of cerebral palsy patients depends on the underlying cause. We retrospectively evaluated the clinical phenotype, abnormalities during pregnancy, and cerebral palsy cause of 384 patients, treated at Charité-Medicine University, between 2015 and 2017. The cause of cerebral palsy was identified in 79.9% of cases. Causes prior to the perinatal period were, compared to perinatal brain damage, associated significantly with different comorbidities. The term cerebral palsy does not describe a single disease but is an umbrella term covering many different diseases. Depending on the cause, a varying clinical phenotype can be found, which offers great potential in terms of individual treatment and preventing comorbidities.
Keywords: cerebral palsy; clinical phenotype; disease cause.
Conflict of interest statement
Figures
References
-
- Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy Dev Med Child Neurol Suppl. 2007;109:8-14. - PubMed
