

The Spillover Effect of the Medicare Mandatory Bundled Payment Program on Joint Replacement Outcomes: Analysis of Patients with Commercial Insurance and Medicare Advantage
- PMID: 34898513
- PMCID: PMC9189235
- DOI: 10.2106/JBJS.21.00259
The Spillover Effect of the Medicare Mandatory Bundled Payment Program on Joint Replacement Outcomes: Analysis of Patients with Commercial Insurance and Medicare Advantage
Abstract
Background: To improve the value and efficiency of care among traditional Medicare enrollees, the Centers for Medicare & Medicaid Services has implemented alternative payment models designed to control health-care spending and improve quality. These models may affect care beyond traditional Medicare enrollees, "spilling over" into other populations. Established in April 2016, the Medicare mandatory bundled payment program, called the Comprehensive Care for Joint Replacement (CJR) model, holds hospitals accountable for spending and quality of care for traditional Medicare joint-replacement patients during care episodes that span from the index hospitalization to 90 days post-discharge. We assessed the extent to which the CJR model was associated with outcomes for patients enrolled in commercial insurance and Medicare Advantage plans.
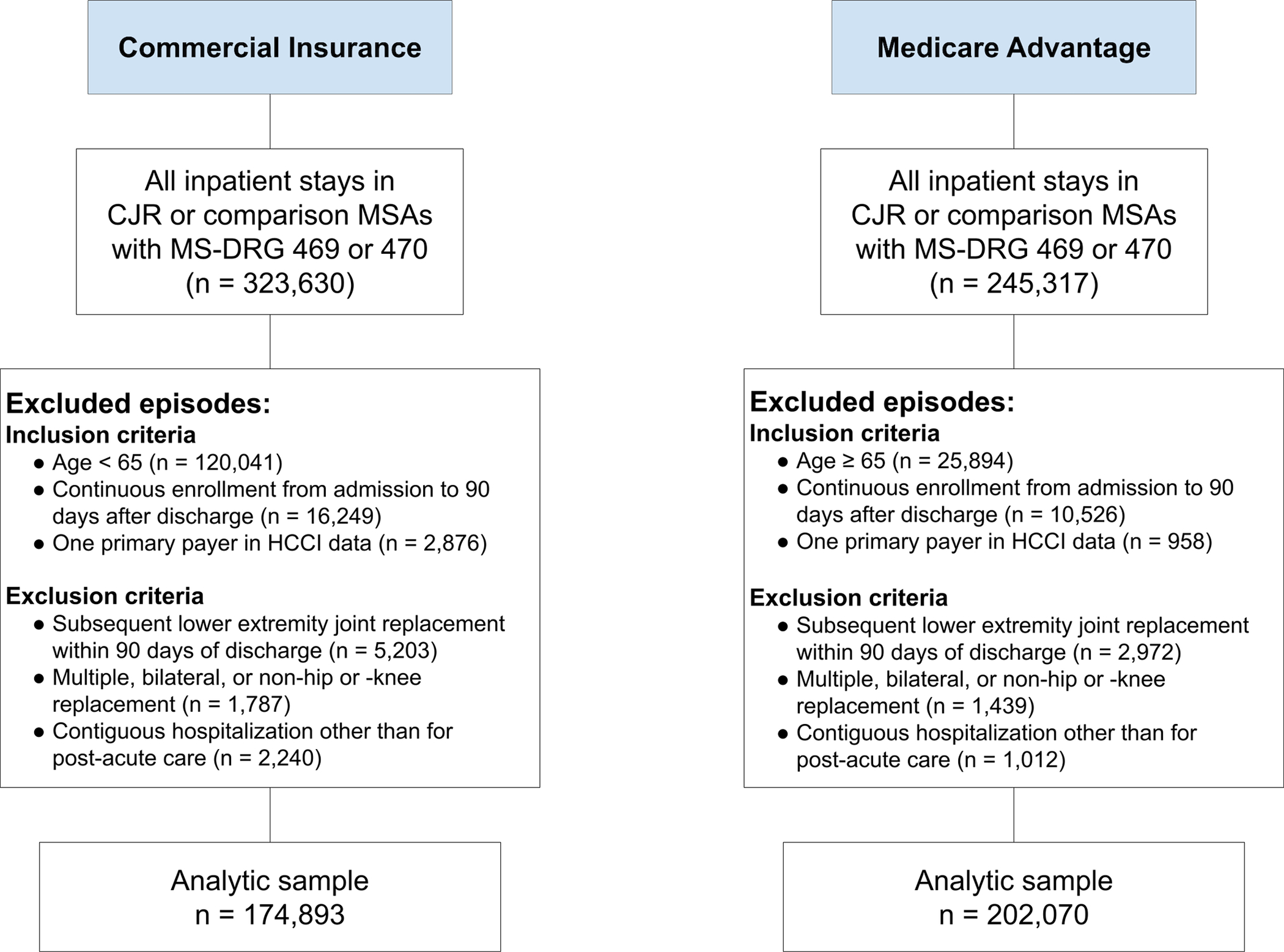
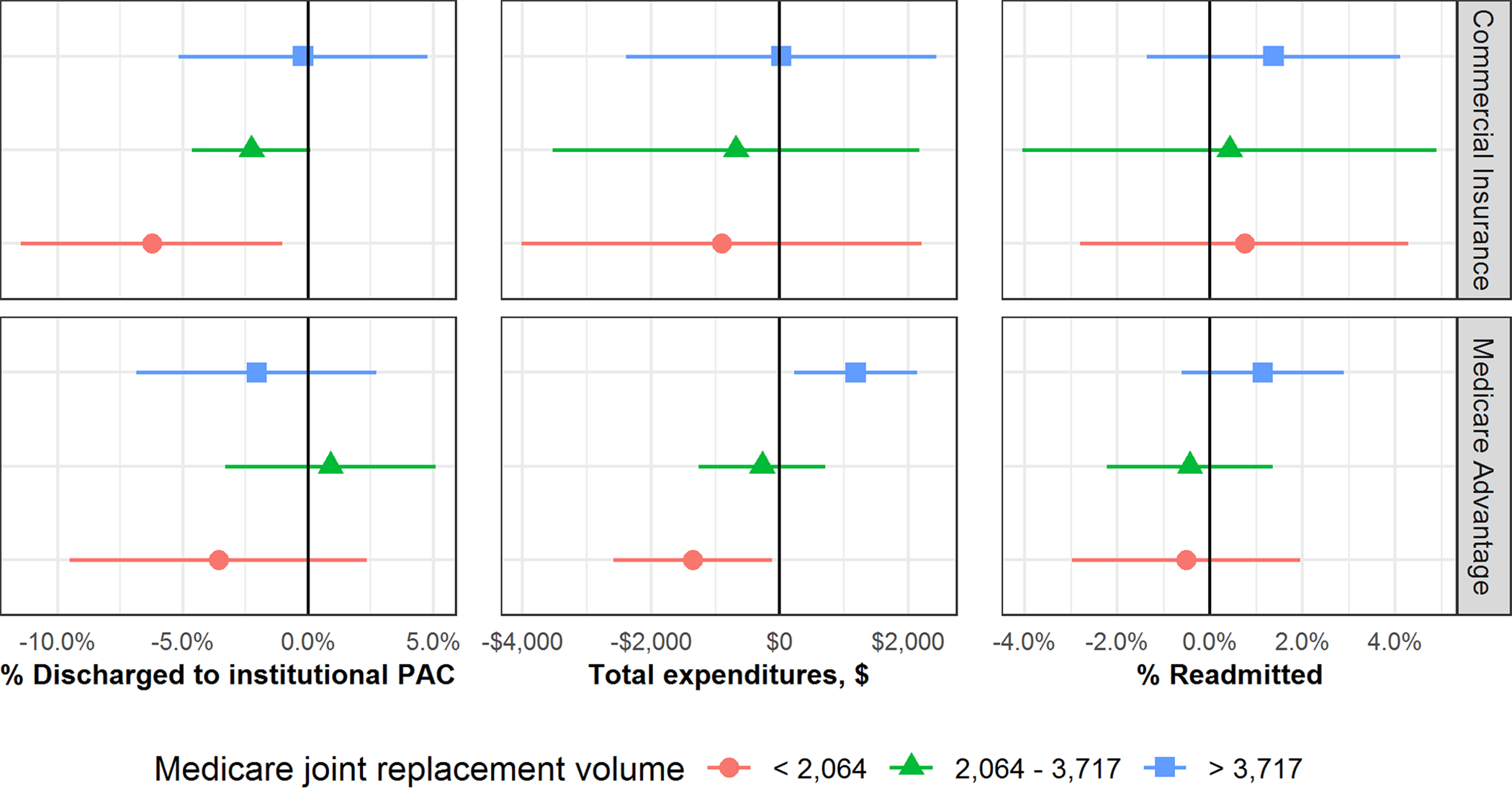
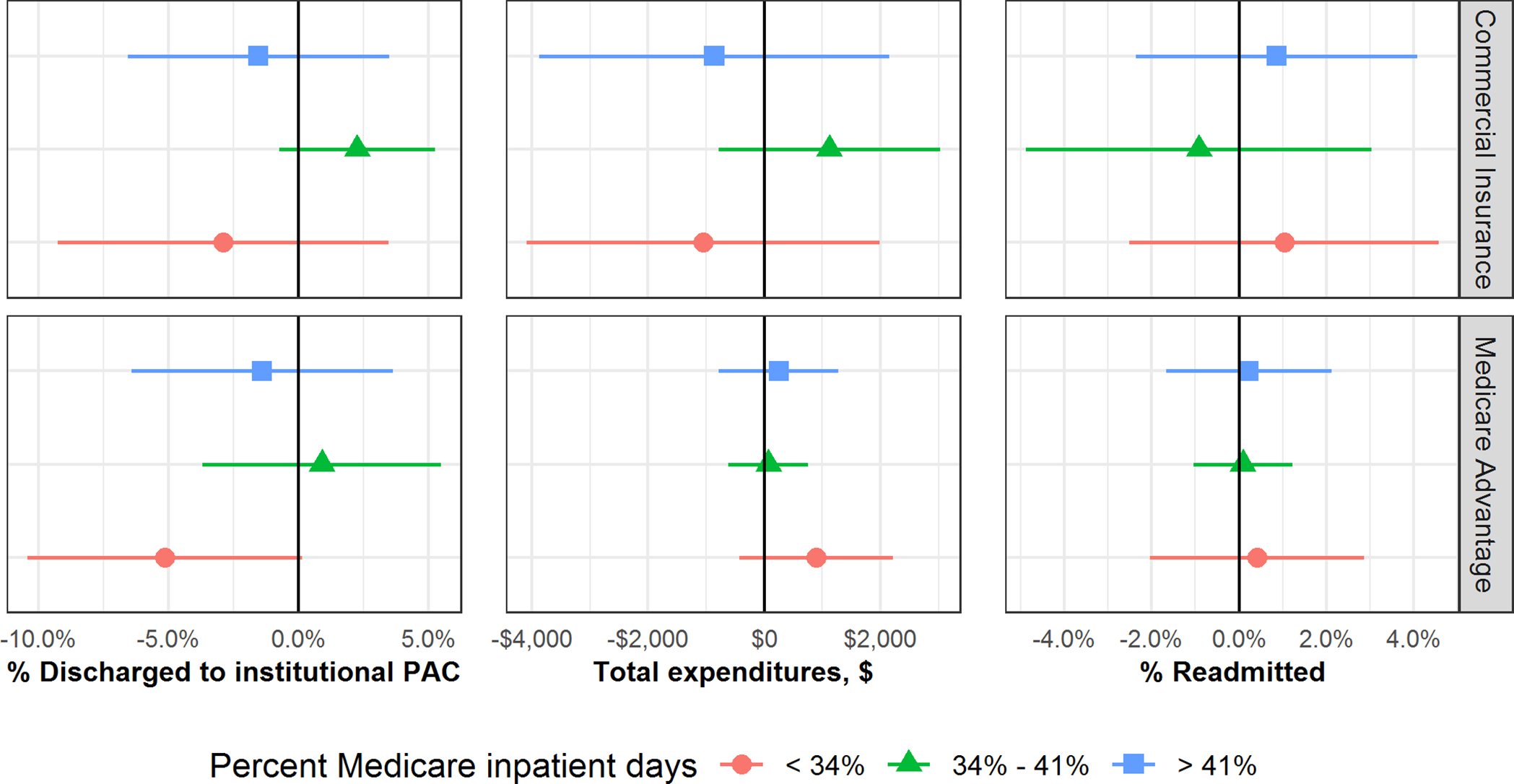
Methods: With use of Health Care Cost Institute claims data from 2012 through 2017, we assessed the association of the CJR model with total expenditures, discharges to institutional post-acute care, and readmissions among commercial insurance and Medicare Advantage joint-replacement patients. The exposure variable was the implementation of the CJR model in 67 randomly selected metropolitan statistical areas compared with 103 similar areas without CJR implementation. We utilized difference-in-differences models to estimate the spillover effects of the CJR model by comparing outcomes between these areas before and after CJR implementation.
Results: The study included 174,893 joint-replacement episodes of care in commercial insurance enrollees and 202,070 episodes in Medicare Advantage enrollees. Among both commercial insurance and Medicare Advantage enrollees, CJR implementation was associated with no meaningful changes in total episode expenditures, discharges to institutional post-acute care, or readmissions.
Conclusions: We found no evidence for spillover effects of the CJR model on commercial insurance and Medicare Advantage patients, suggesting that alternative payment models targeting traditional Medicare patients may have limited effects on the cost and quality of care for patients outside of the traditional Medicare system.
Copyright © 2021 by The Journal of Bone and Joint Surgery, Incorporated.
Conflict of interest statement
Disclosure: The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article ( http://links.lww.com/JBJS/G825 ).
Figures
References
-
- Navathe AS, Boyle CW, Emanuel EJ. Alternative Payment Models-Victims of Their Own Success? JAMA. 2020. Jul 21;324(3):237–8. - PubMed
-
- Centers for Medicare and Medicaid Services. Comprehensive Care for Joint Replacement Model. 2020. Accessed 2021 Nov 10. https://innovation.cms.gov/initiatives/cjr
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
