

The More, the Merrier…? Antipsychotic Polypharmacy Treatment Strategies in Schizophrenia From a Pharmacology Perspective
- PMID: 34899422
- PMCID: PMC8652414
- DOI: 10.3389/fpsyt.2021.760181
The More, the Merrier…? Antipsychotic Polypharmacy Treatment Strategies in Schizophrenia From a Pharmacology Perspective
Abstract
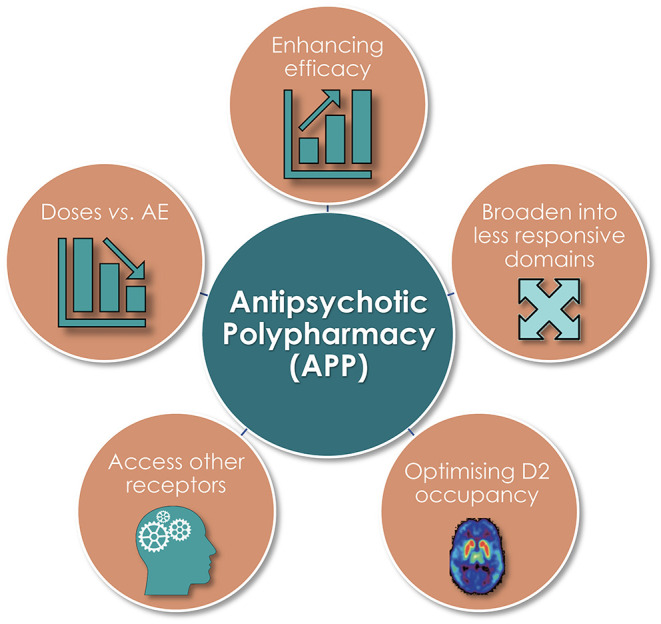
Antipsychotic polypharmacy/drug combination treatment (APP) is a remarkably common practice in the schizophrenia context, given the lack of general support in treatment Guidelines. There is also a vast literature on APP outcomes, but a paucity of high-quality evidence-based data to guide and optimize adequate use of APP. This seems particularly true regarding many pharmacology-based considerations involved in APP treatment strategies. This paper first briefly summarizes clinical literature related to the use of APP. Against this backdrop, the pharmacological target profile features are then described of frequently used antipsychotic agents, in relation to estimated free plasma exposure levels at clinically efficacious dosing. APP strategies based on the properties of these drugs are then scrutinized and gauged within the background literature framework. The anticipated usefulness of APP from the pharmacological standpoint is detailed regarding efficacy, adverse effect (AE)/tolerability, and safety perspective, including why, when, and how it may be used to its advantage. For the purpose, a number of theoretically beneficial combinations as well as instances with suboptimal-and even futile-APP approaches are exemplified and discussed from the rational pharmacodynamic and pharmacokinetic pros and cons point-of-view. In this exposé, particular attention is paid to the utility and features of 3rd Generation Antipsychotic dopamine (DA) D2-D3 agonists within an APP setting.
Keywords: adverse events; antipsychotics; drug combinations; efficacy; pharmacodynamic profiles; polypharmacy; pros and cons; schizophrenia.
Copyright © 2021 Hjorth.
Conflict of interest statement
Over the last 3 years, SH has received honoraria from Lundbeck, Otsuka, Gedeon Richter, and Recordati for scientific talks and/or participation in advisory boards. He does not hold any shares or has financial interest in any of the companies marketing the antipsychotic agents discussed in the paper. SH is a self-employed independent consultant with his own company Pharmacilitator AB (Inc.).
Figures






References
-
- NICE . NICE Guideline: Psychosis and Schizophrenia in Adults: Prevention and Management. In: Clinical guideline (CG). NICE (National Institute for Health and Care Excellence). (2014). Available online at: www.nice.org.uk/guidance/cg178 (accessed October 29, 2021).
LinkOut - more resources
Full Text Sources
Miscellaneous