

Functional Recovery and Serum Angiogenin Changes According to Intensity of Rehabilitation Therapy After Stroke
- PMID: 34899582
- PMCID: PMC8655101
- DOI: 10.3389/fneur.2021.767484
Functional Recovery and Serum Angiogenin Changes According to Intensity of Rehabilitation Therapy After Stroke
Abstract
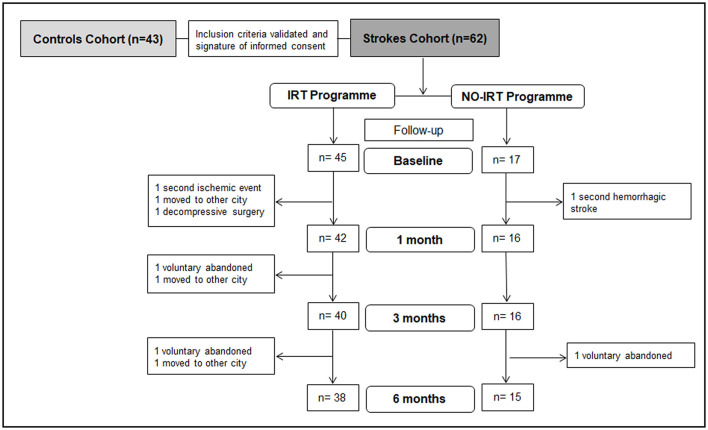
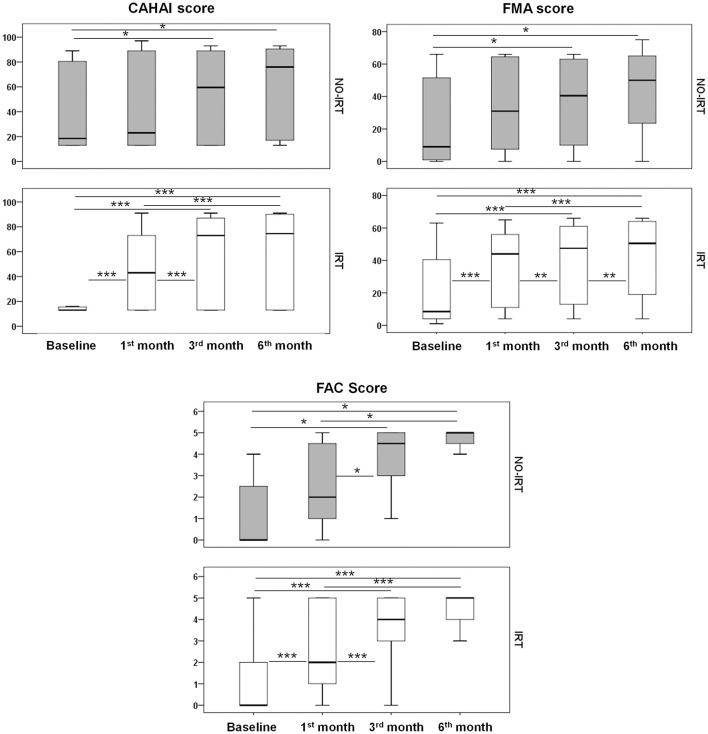
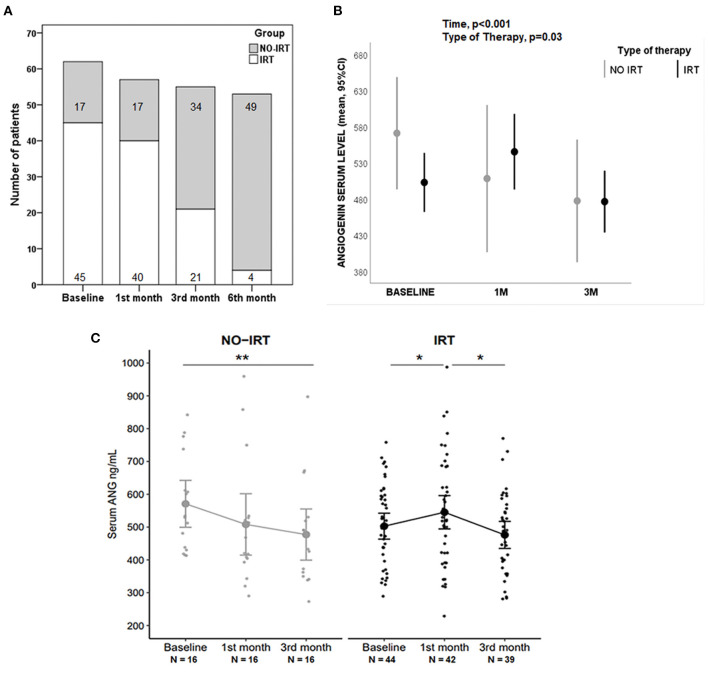
Background: Rehabilitation is still the only treatment available to improve functional status after the acute phase of stroke. Most clinical guidelines highlight the need to design rehabilitation treatments considering starting time, intensity, and frequency, according to the tolerance of the patient. However, there are no homogeneous protocols and the biological effects are under investigation. Objective: To investigate the impact of rehabilitation intensity (hours) after stroke on functional improvement and serum angiogenin (ANG) in a 6-month follow-up study. Methods: A prospective, observational, longitudinal, and multicenter study with three cohorts: strokes in intensive rehabilitation therapy (IRT, minimum 15 h/week) vs. conventional therapy (NO-IRT, <15 h/week), and controls subjects (without known neurological, malignant, or inflammatory diseases). A total of seven centers participated, with functional evaluations and blood sampling during follow-up. The final cohort includes 62 strokes and 43 controls with demographic, clinical, blood samples, and exhaustive functional monitoring. Results: The median (IQR) number of weekly hours of therapy was different: IRT 15 (15-16) vs. NO-IRT 7.5 (5-9), p < 0.01, with progressive and significant improvements in both groups. However, IRT patients showed earlier improvements (within 1 month) on several scales (CAHAI, FMA, and FAC; p < 0.001) and the earliest community ambulation achievements (0.89 m/s at 3 months). There was a significant difference in ANG temporal profile between the IRT and NO-IRT groups (p < 0.01). Additionally, ANG was elevated at 1 month only in the IRT group (p < 0.05) whereas it decreased in the NO-IRT group (p < 0.05). Conclusions: Our results suggest an association of rehabilitation intensity with early functional improvements, and connect the rehabilitation process with blood biomarkers.
Keywords: angiogenin; biomarker; intensive therapy; recovery; rehabilitation.
Copyright © 2021 Garcia-Rodriguez, Rodriguez, Tejada, Miranda-Artieda, Ridao, Buxó, Pérez-Mesquida, Beseler, Salom, Pérez, Inzitari, Otero-Villaverde, Martin-Mourelle, Molleda, Quintana, Olivé-Gadea, Penalba and Rosell.
Conflict of interest statement
LP and MI have received honoraria from Nestlé for activities unrelated to the present work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous