

Robust Antibody Levels in Both Diabetic and Non-Diabetic Individuals After BNT162b2 mRNA COVID-19 Vaccination
- PMID: 34899701
- PMCID: PMC8652288
- DOI: 10.3389/fimmu.2021.752233
Robust Antibody Levels in Both Diabetic and Non-Diabetic Individuals After BNT162b2 mRNA COVID-19 Vaccination
Abstract
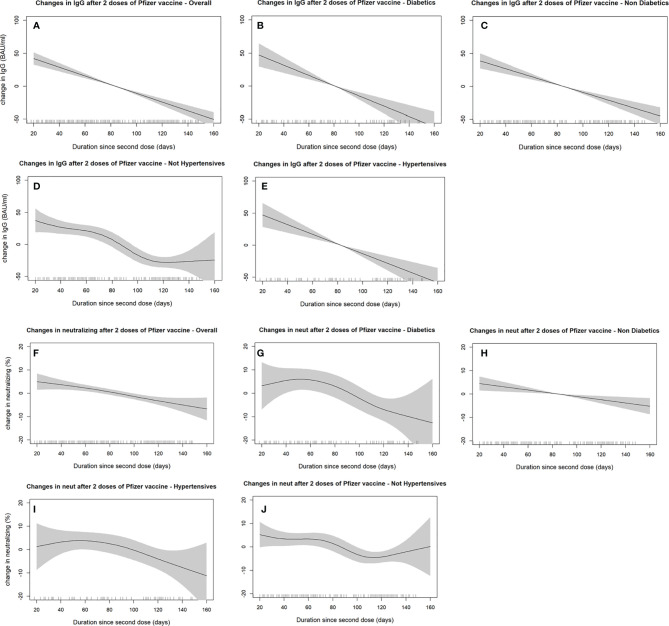
The emergence of effective vaccines for COVID-19 has been welcomed by the world with great optimism. Given their increased susceptibility to COVID-19, the question arises whether individuals with type-2 diabetes mellitus (T2DM) and other metabolic conditions can respond effectively to the mRNA-based vaccine. We aimed to evaluate the levels of anti-SARS-CoV-2 IgG and neutralizing antibodies in people with T2DM and/or other metabolic risk factors (hypertension and obesity) compared to those without. This study included 262 people (81 diabetic and 181 non-diabetic persons) that took two doses of BNT162b2 (Pfizer-BioNTech) mRNA vaccine. Both T2DM and non-diabetic individuals had a robust response to vaccination as demonstrated by their high antibody titers. However, both SARS-CoV-2 IgG and neutralizing antibodies titers were lower in people with T2DM. The mean ( ± 1 standard deviation) levels were 154 ± 49.1 vs. 138 ± 59.4 BAU/ml for IgG and 87.1 ± 11.6 vs. 79.7 ± 19.5% for neutralizing antibodies in individuals without diabetes compared to those with T2DM, respectively. In a multiple linear regression adjusted for individual characteristics, comorbidities, previous COVID-19 infection, and duration since second vaccine dose, diabetics had 13.86 BAU/ml (95% CI: 27.08 to 0.64 BAU/ml, p=0.041) less IgG antibodies and 4.42% (95% CI: 8.53 to 0.32%, p=0.036) fewer neutralizing antibodies than non-diabetics. Hypertension and obesity did not show significant changes in antibody titers. Taken together, both type-2 diabetic and non-diabetic individuals elicited strong immune responses to SARS-CoV-2 BNT162b2 mRNA vaccine; nonetheless, lower levels were seen in people with diabetes. Continuous monitoring of the antibody levels might be a good indicator to guide personalized needs for further booster shots to maintain adaptive immunity. Nonetheless, it is important that people get their COVID-19 vaccination especially people with diabetes.
Keywords: BNT162b2; COVID-19; COVID-19 vaccine; T2D; antibodies; diabetes mellitus type 2; mRNA vaccine; vaccine.
Copyright © 2021 Ali, Alterki, Sindhu, Alahmad, Hammad, Al-Sabah, Alghounaim, Jamal, Aldei, Mairza, Husain, Deverajan, Ahmad, Cherian, Alkhairi, Alkandari, Abubaker, Abu-Farha and Al-Mulla.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous