

Strategies to Improve the Antitumor Effect of Immunotherapy for Hepatocellular Carcinoma
- PMID: 34899747
- PMCID: PMC8660685
- DOI: 10.3389/fimmu.2021.783236
Strategies to Improve the Antitumor Effect of Immunotherapy for Hepatocellular Carcinoma
Abstract
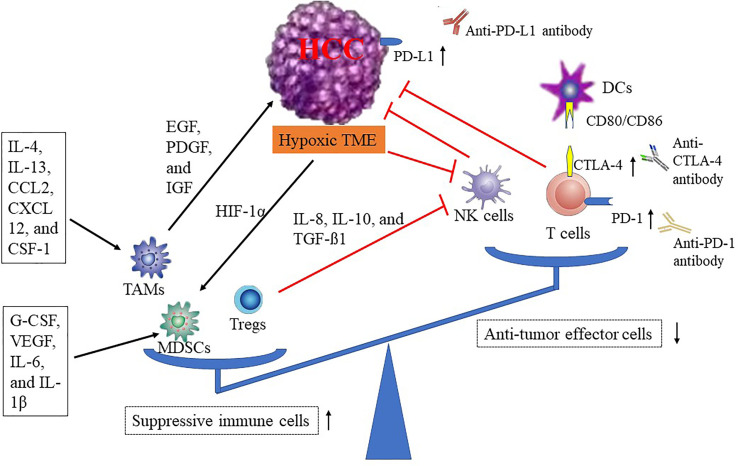
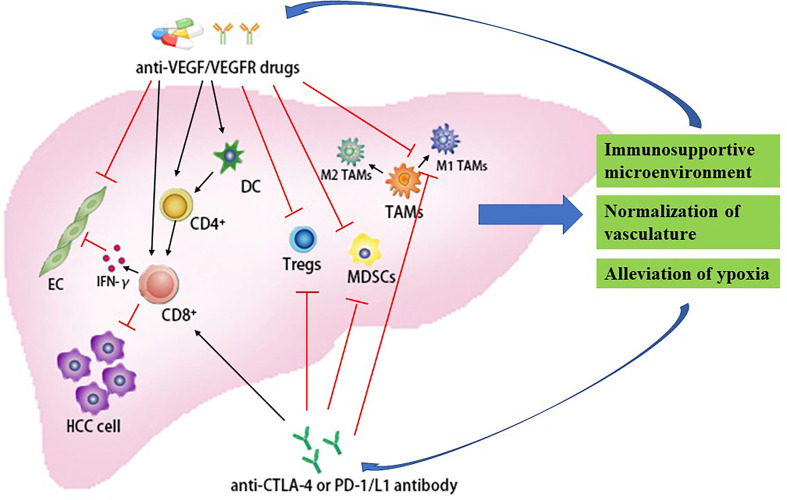
Hepatocellular carcinoma (HCC), one of the most fatal malignancies in the world, is usually diagnosed in advanced stages due to late symptom manifestation with very limited therapeutic options, which leads to ineffective intervention and dismal prognosis. For a decade, tyrosine kinase inhibitors (TKIs) have offered an overall survival (OS) benefit when used in a first-line (sorafenib and lenvatinib) and second-line setting (regorafenib and cabozantinib) in advanced HCC, while long-term response remains unsatisfactory due to the onset of primary or acquired resistance. Recently, immunotherapy has emerged as a promising therapy in the treatment of several solid tumors, such as melanoma and non-small cell lung cancer. Moreover, as the occurrence of HCC is associated with immune tolerance and immunosurveillance escape, there is a potent rationale for employing immunotherapy in HCC. However, immunotherapy monotherapy, mainly including immune checkpoint inhibitors (ICIs) that target checkpoints programmed death-1 (PD-1), programmed death-ligand 1 (PD-L1), and the cytotoxic T lymphocyte antigen-4 (CTLA-4), has a relatively low response rate. Thus, the multi-ICIs or the combination of immunotherapy with other therapies, like antiangiogenic drugs and locoregional therapies, has become a novel strategy to treat HCC. Combining different ICIs may have a synergistical effect attributed to the complementary effects of the two immune checkpoint pathways (CTLA-4 and PD-1/PD-L1 pathways). The incorporation of antiangiogenic drugs in ICIs can enhance antitumor immune responses via synergistically regulating the vasculature and the immune microenvironment of tumor. In addition, locoregional treatments can improve antitumor immunity by releasing the neoplasm antigens from killed tumor cells; in turn, this antitumor immune response can be intensified by immunotherapy. Therefore, the combination of locoregional treatments and immunotherapy may achieve greater efficacy through further synergistic effects for advanced HCC. This review aims to summarize the currently reported results and ongoing trials of the ICIs-based combination therapies for HCC to explore the rational combination strategies and further improve the survival of patients with HCC.
Keywords: antiangiogenic drugs; combination therapy; hepatocellular carcinoma; immune checkpoint inhibitors; locoregional therapies.
Copyright © 2021 Xing, Gao, Cui and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials