

Cobimetinib Plus Gemcitabine: An Active Combination in KRAS G12R-Mutated Pancreatic Ductal Adenocarcinoma Patients in Previously Treated and Failed Multiple Chemotherapies
- PMID: 34901697
- PMCID: PMC8655806
- DOI: 10.1089/pancan.2021.0006
Cobimetinib Plus Gemcitabine: An Active Combination in KRAS G12R-Mutated Pancreatic Ductal Adenocarcinoma Patients in Previously Treated and Failed Multiple Chemotherapies
Abstract
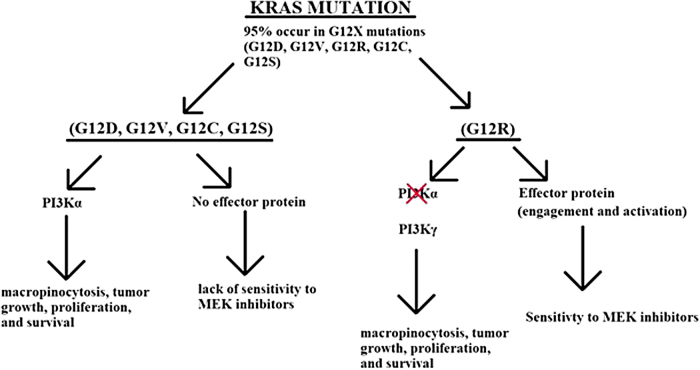
Purpose: The KRAS proto-oncogene is involved in the RAS/MAPK pathway. KRAS is present in the wild type or mutated forms. The oncogene KRAS is frequently mutated in various cancers. At the time that amino acid glycine is mutated, KRAS protein acquires oncogenic properties that result in the tumor cell growth, proliferation, and cancer progression. There has been limited understanding of the different mutations at codon 12. The consequences of such mutations is not fully understood. Various G12X mutations in pancreatic cancer patients have been examined, with the most common mutations being G12D (40%), G12V (30%), and G12R (15-20%). Now we are understanding that G12X mutations in the KRAS are not all equal. Methods: In a single-arm exploratory study, we accrued 13 KRAS-G12X-mutated pancreatic patients (KRAS G12D, G12V, and G12R). They were divided into two groups: group 1 consisted of seven patients with G12D and G12V and group 2 included six patients with the KRAS G12R mutation. All patients were treated with the combination of gemcitabine at 1250 mg/m2 intravenous weekly for 3 weeks and oral cobimetinib 20 mg b.i.d. for 3 weeks. This was followed by a week of rest before the initiation of the next cycle. Results: In the first cohort, seven patients were on treatment, all of whom progressed and died within the 2 months of the study. In the second cohort, one of six patients achieved partial response, and five achieved stable disease. Median progression-free survival was 6 months (9% confidence interval 3.0-9.3 months) and overall survival has been reached at 8 months. Common adverse reactions included rash, fatigue, nausea, and vomiting (grades 2 and 3). Cancer antigen CA19-9 decreased by >50% in all group 2 patients. Conclusion: Our pancreatic cancer patients were heavily pretreated (all had received FOLFIRINOX and gemcitabine/nab-paclitaxel) before the entry into our trial. Upon entry into our trial, all patients were treated with the combination of gemcitabine and oral cobimetinib. Therefore, this constituted the second exposure of the patients to gemcitabine. This study illustrates a new discovery, which can potentially target 15-20% of pancreatic cancer patients and allow for a significant improvement in their prognosis. We will be conducting randomized phase II trials to substantiate our findings.
Keywords: KRAS G12R; KRAS-mutant; MEK inhibitor; next-generation sequencing; pancreatic cancer.
© Bach Ardalan et al., 2021; Published by Mary Ann Liebert, Inc.
Conflict of interest statement
The authors declare that there is no competing interests, potential or actual, and financial or other.
Figures
References
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–1825. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous