

Standardized two-step testing of antibody activity in COVID-19 convalescent plasma
- PMID: 34901783
- PMCID: PMC8653399
- DOI: 10.1016/j.isci.2021.103602
Standardized two-step testing of antibody activity in COVID-19 convalescent plasma
Abstract
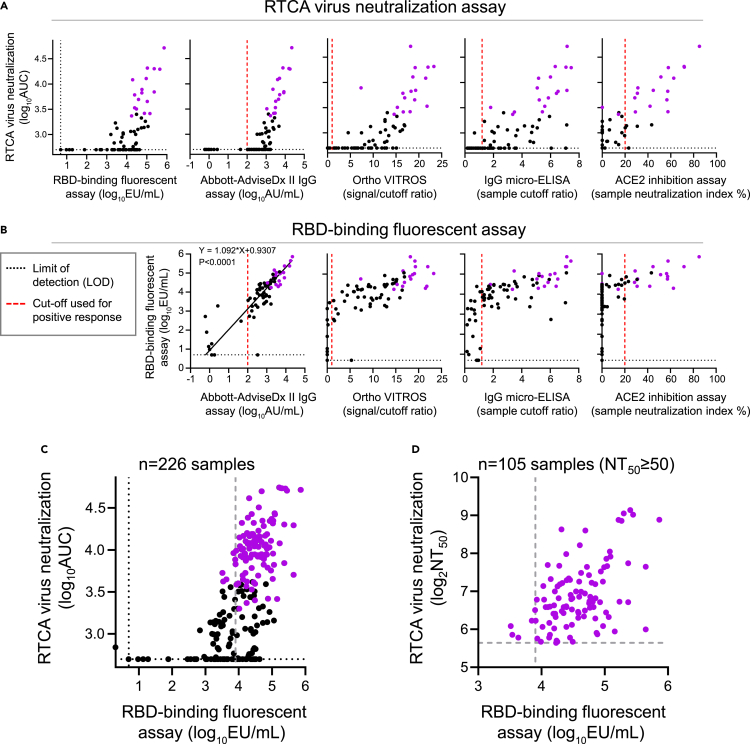
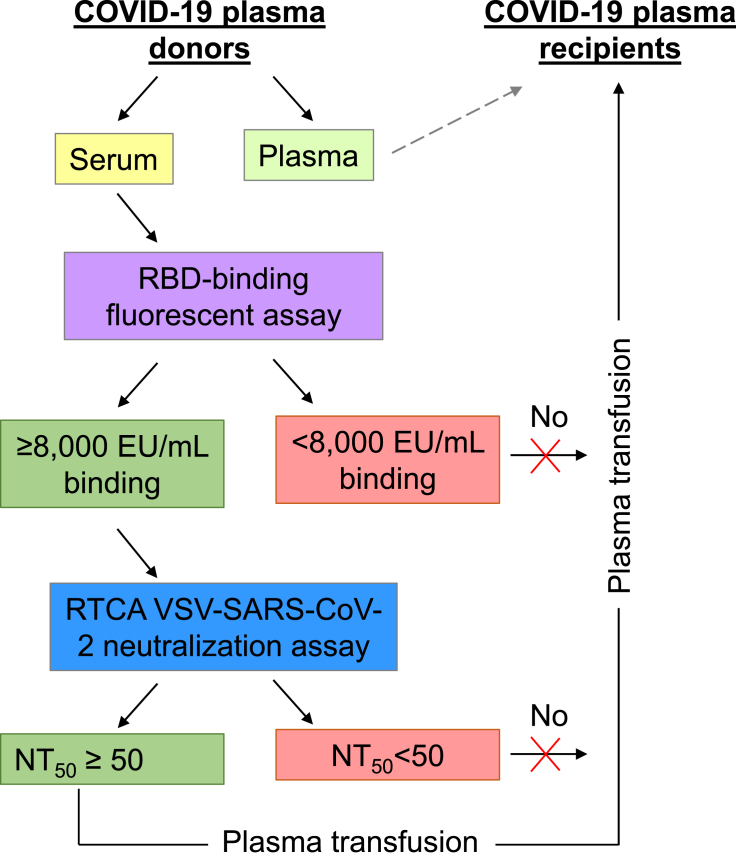
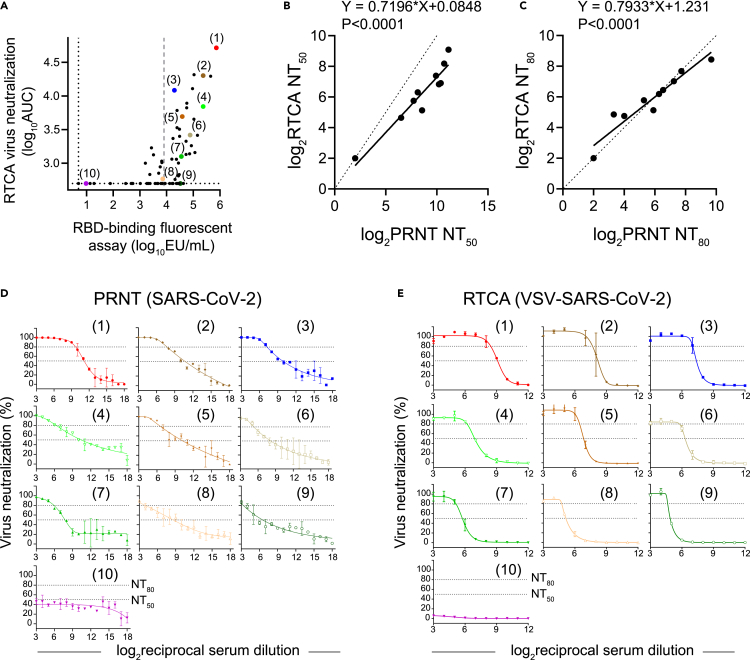
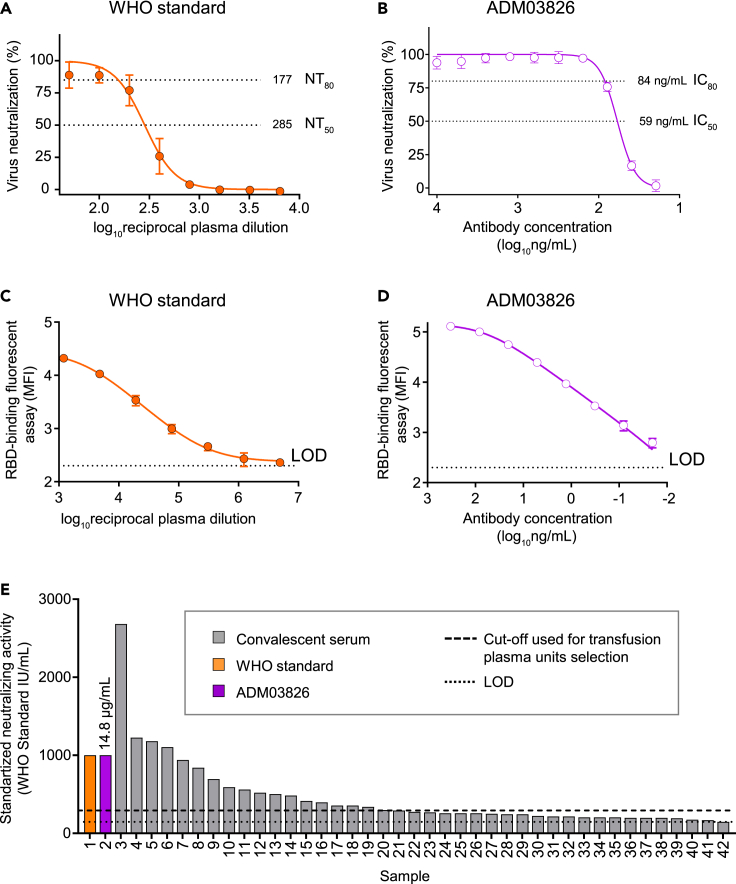
The COVID-19 pandemic revealed an urgent need for rapid profiling of neutralizing antibody responses and development of antibody therapeutics. The current Food and Drug Administration-approved serological tests do not measure antibody-mediated viral neutralization, and there is a need for standardized quantitative neutralization assays. We report a high-throughput two-step profiling approach for identifying neutralizing convalescent plasma. Screening and downselection for serum antibody binding to the receptor-binding domain are followed by quantitative neutralization testing using a chimeric vesicular stomatitis virus expressing spike protein of SARS-CoV-2 in a real-time cell analysis assay. This approach enables a predictive screening process for identifying plasma units that neutralize SARS-CoV-2. To calibrate antibody neutralizing activity in serum from convalescent plasma donors, we introduce a neutralizing antibody standard reagent composed of two human antibodies that neutralize SARS-CoV strains, including SARS-CoV-2 variants of concern. Our results provide a framework for establishing a standardized assessment of antibody-based interventions against COVID-19.
Keywords: Immunology; Virology.
© 2021 The Authors.
Conflict of interest statement
I.T. reports grants from NIH/NIAID, during the conduct of the study, and has served as a consultant for Nashville Biosciences and Horizon Therapeutics. J. D. C., L.J.S., and M.R.D. report grants from NIH/NCATS, during the conduct of the study. T.W.R. reports grants from NIH/NCATS, during the conduct of the study; personal fees from Cumberland Pharmaceuticals, Inc, personal fees from Sanofi Pharma, and personal fees from Cytovale, outside the submitted work. T.G.S. reports grants from NIH, during the conduct of the study. W.H.S. reports grants from NCATS of the NIH, during the conduct of the study. M.S.D. is a consultant for Inbios, Vir Biotechnology, Fortress Biotech, and Carnival Corporation and on the Scientific Advisory Boards of Moderna and Immunome. The Diamond laboratory has received funding support in sponsored research agreements from Moderna, Vir Biotechnology, and Emergent BioSolutions. J.E.C. has served as a consultant for Luna Biologics, is a member of the Scientific Advisory Board of Meissa Vaccines and is Founder of IDBiologics. The Crowe laboratory at Vanderbilt University Medical Center has received sponsored research agreements from Takeda Vaccines, IDBiologics, and AstraZeneca and grants from NIH, and DARPA during the conduct of the study. Vanderbilt University has applied for patents related to antibodies described in this paper. All other authors declare no competing interests.
Figures



References
-
- Addetia A., Crawford K.H.D., Dingens A., Zhu H., Roychoudhury P., Huang M.L., Jerome K.R., Bloom J.D., Greninger A.L. Neutralizing antibodies correlate with protection from SARS-CoV-2 in humans during a fishery vessel outbreak with a high attack rate. J. Clin. Microbiol. 2020;58:e02107–e02120. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
