

Inequalities in developing multimorbidity over time: A population-based cohort study from an urban, multi-ethnic borough in the United Kingdom
- PMID: 34901910
- PMCID: PMC8640725
- DOI: 10.1016/j.lanepe.2021.100247
Inequalities in developing multimorbidity over time: A population-based cohort study from an urban, multi-ethnic borough in the United Kingdom
Abstract
Background: Social and material deprivation accelerate the development of multimorbidity, yet the mechanisms which drive multimorbidity pathways and trajectories remain unclear. We aimed to examine the association between health inequality, risk factors and accumulation or resolution of LTCs, taking disease sequences into consideration.
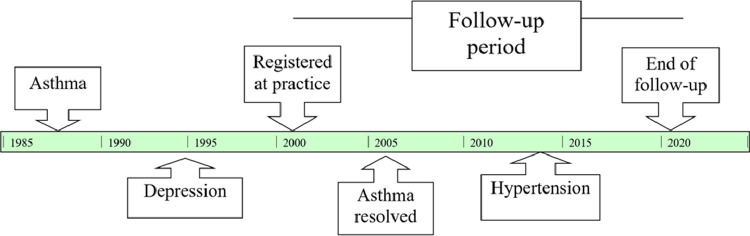
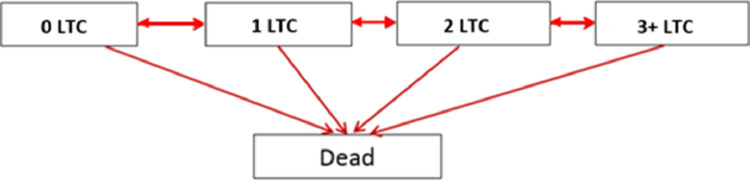
Methods: We conducted a retrospective cohort of adults aged 18 years and over, registered between April 2005 and May 2020 in general practices in one inner London borough (n = 826,936). Thirty-two long term conditions (LTCs) were selected using a consensus process, based on a definition adapted to the demographic characteristics of the local population. sThe development and resolution of these LTCs were examined according to sociodemographic and clinical risk factors (hypertension; moderate obesity (BMI 30·0-39·9 kg/m2), high cholesterol (total cholesterol > 5 mmol/L), smoking, high alcohol consumption (>14 units per week), and psychoactive substance use), through the application of multistate Markov chain models.
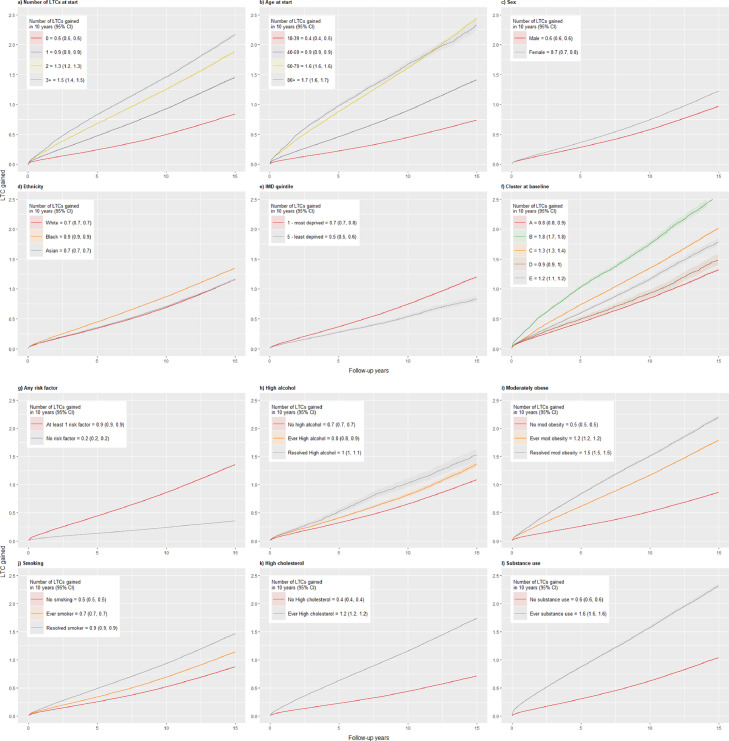
Findings: Participants were followed up for a median of 4.2 years (IQR = 1·8 - 8·4); 631,760 (76%) entered the study with no LTCs, 121,424 (15%) with 1 LTC, 41,720 (5%) with 2 LTCs, and 31,966 (4%) with three or more LTCs. At the end of follow-up, 194,777 (24%) gained one or more LTCs, while 45,017 (5%) had resolved LTCs and 27,021 (3%) died. In multistate models, deprivation (hazard ratio [HR] between 1·30 to 1·64), female sex (HR 1·13 to 1·20), and Black ethnicity (HR 1·20 to 1·30; vs White) were independently associated with increased risk of transition from one to two LTCs, and shorter time spent in a healthy state. Substance use was the strongest risk factor for multimorbidity with an 85% probability of gaining LTCs over the next year. First order Markov chains identified consistent disease sequences including: chronic pain or osteoarthritis followed by anxiety and depression; alcohol and substance dependency followed by HIV, viral hepatitis, and liver disease; and morbid obesity followed by diabetes, hypertension, and chronic pain.
Interpretation: We examined the relations among 32 LTCs, taking the order of disease occurrence into consideration. Distinctive patterns for the development and accumulation of multimorbidity have emerged, with increased risk of transitioning from no conditions to multimorbidity and mortality related to ethnicity, deprivation and gender. Musculoskeletal disorders, morbid obesity and substance abuse represent common entry points to multimorbidity trajectories.
Keywords: IMD, Indices of Multiple Deprivation; LTC, Long term conditions; Long term conditions; MCF, Mean cumulative function; Multi state markov chain; Multimorbidity; Probabilities; QOF, Quality Outcomes Framework; UK, United Kingdom.
© 2021 The Authors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nunes B.P., Flores T.R., Mielke G.I., et al. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2016 DOI: S0167-4943(16)30138-8 [pii] - PubMed
-
- Makovski T.T., Schmitz S., Zeegers M.P., et al. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. 2019 DOI: S1568-1637(19)30006-6 [pii] - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
